Definition
- The development of lesions in vessel intimal wall
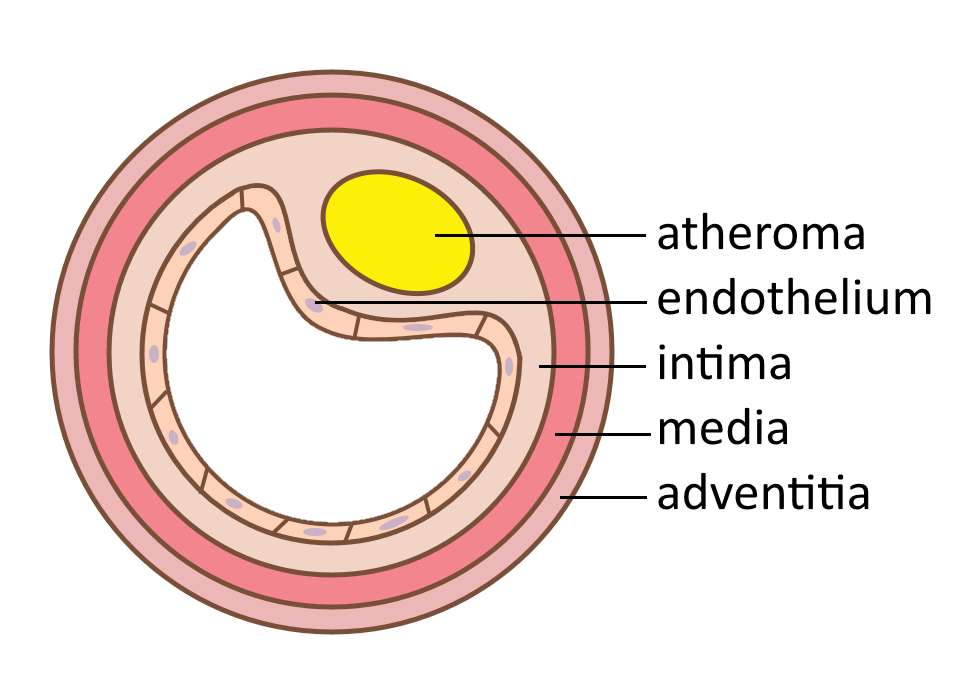
- Known as atherosclerotic plaques or atheromas
- Within intima of large and medium-sized vessels
- Grows over decades to physically obstruct vessels
- Prone to thrombogenic rupture
- Weakens vessel wall, leads to aneurysm
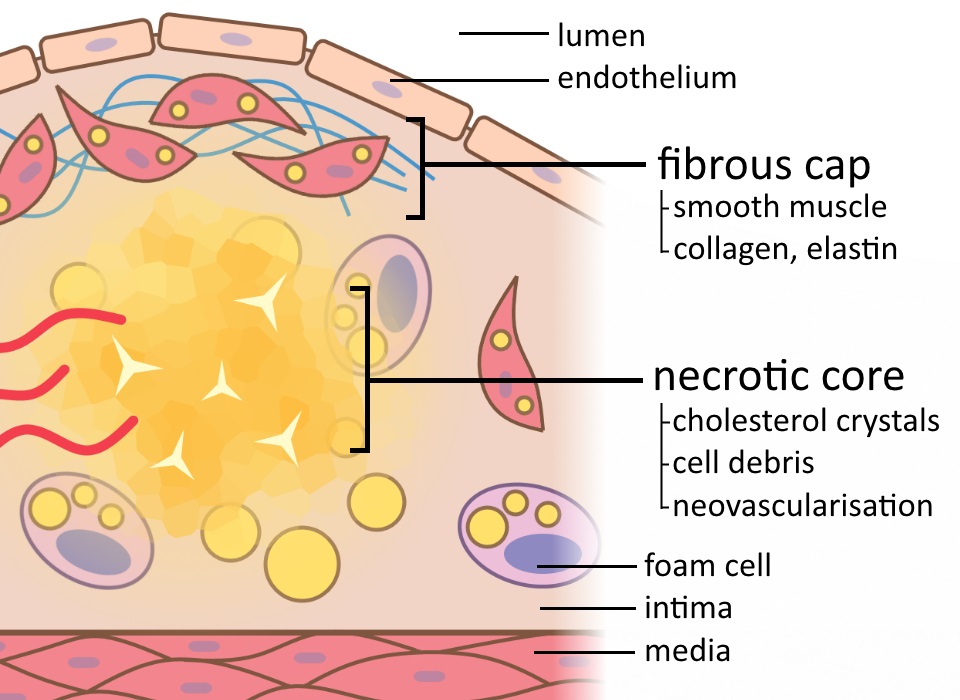
- Composition:
- inflammatory and immune cells
- smooth muscle cells, connective tissue
- lipid, cholesterol

Prevalence
- Extremely common in the Western world
- Leading cause of morbidity and mortality

- Incidence increasing for past 50 years
- Now peaked and declining in some areas (e.g. US)
- Still rising elsewhere (e.g. Japan)
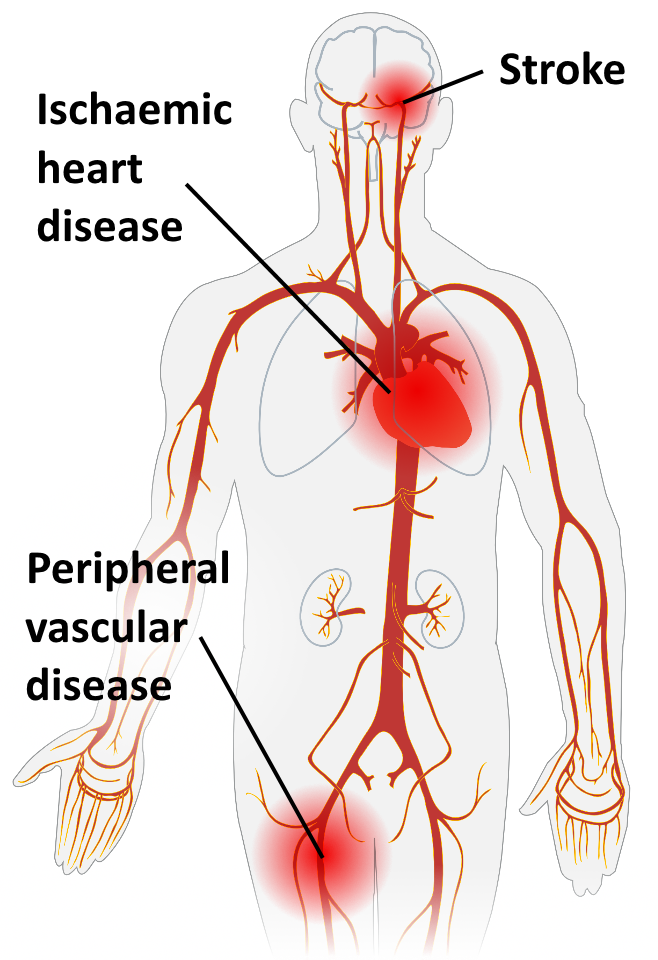
Morbidity
- Responsible for 18% of all DALYs lost in the West
-
Ischaemic heart disease
- angina
- myocardial infarction
-
Stroke
-
severe, long-term disability
-
Peripheral arterial disease
-
pain, cyanosis
-
ulceration, gangrene
Mortality
- Most common cause of Western death
- Implicated in 50% of all deaths
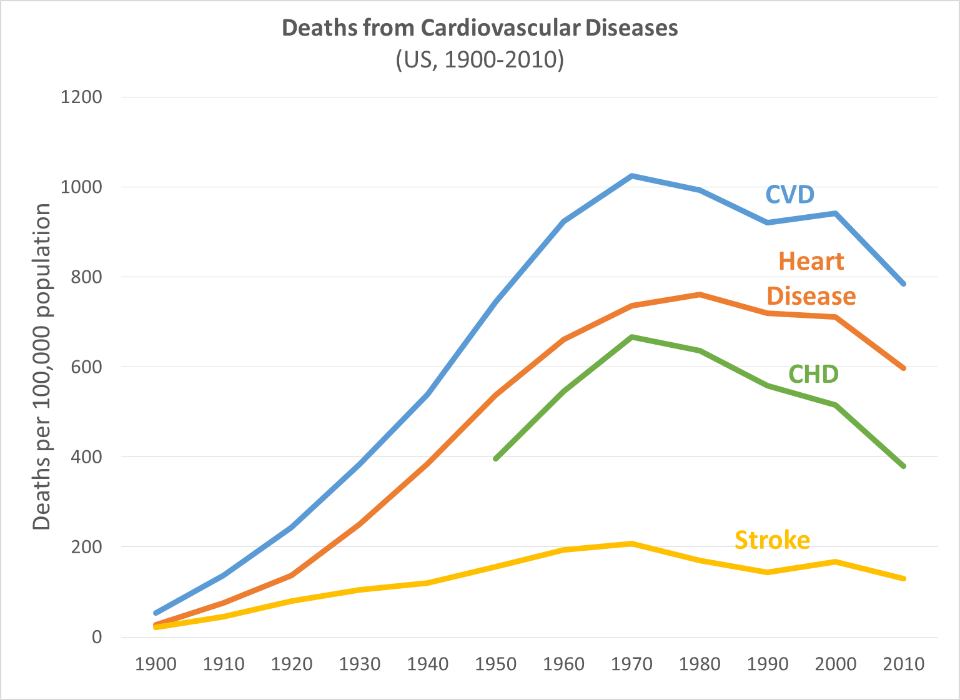
Data: NHLBI
Cost
|
Direct costs: primary care, clinical care, rehabilitation |
$26 billion |
|
Indirect costs: lost productivity due to death and disability |
$48 billion |
| Average cost per case | $82,000 |
Pathogenesis
- A lesion slowly developing over 20-30 years
- May see initial stages (fatty streaks) in childhood
- Risk factors accelerate progression
- Chronic pathogenesis with acute complications
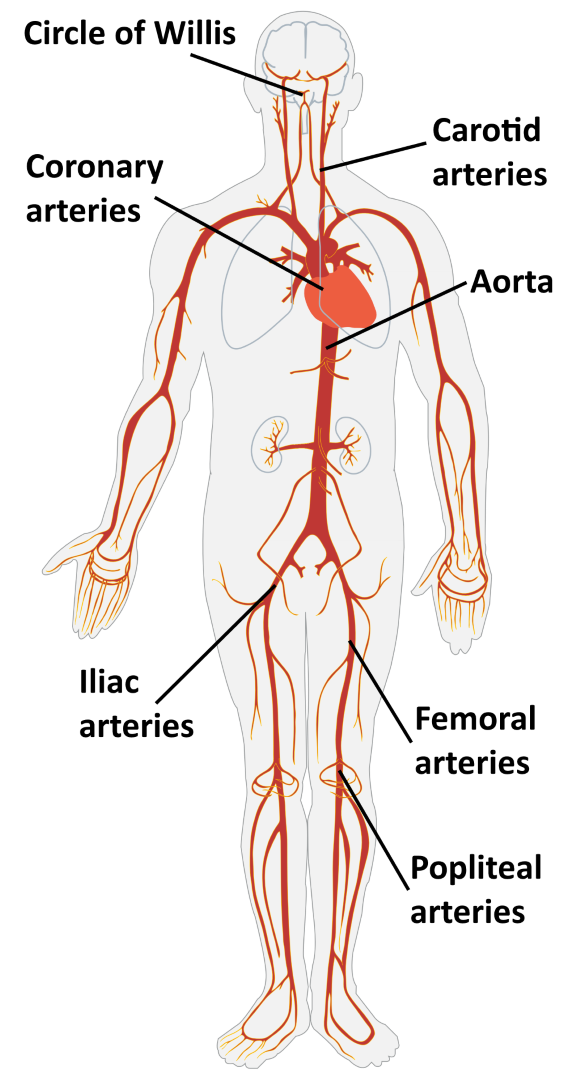
Distribution
- Large and medium arteries only
- Often at turbulent branch points
Common sites:
- Aorta
- Coronary arteries
- Iliac, femoral, popliteal arteries
- Carotid arteries
- Circle of Willis
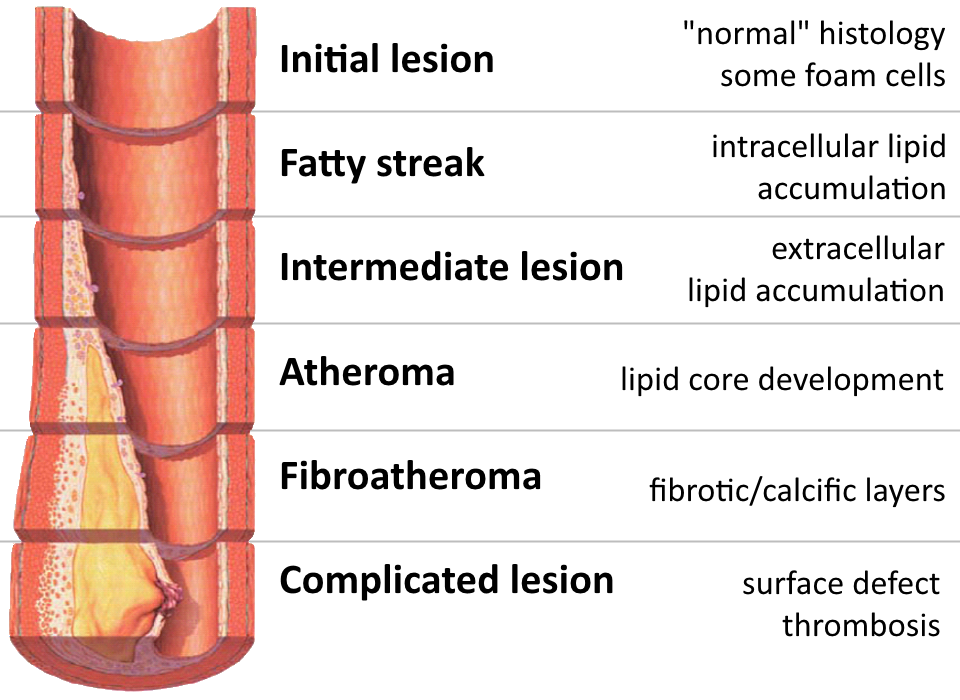
Summary of Events
- Endothelial injury
- Endothelial dysfunction
- monocyte and platelet adhesion
- LDL permeability and uptake
- Engulfment
- of lipids by monocytes and smooth muscle
- foam cell formation
- Proliferation of smooth muscle cells
- fibrous cap generation
- increasing size, vessel stenosis
- Neovascularisation
- potential for haemorrhage
Endothelial Injury
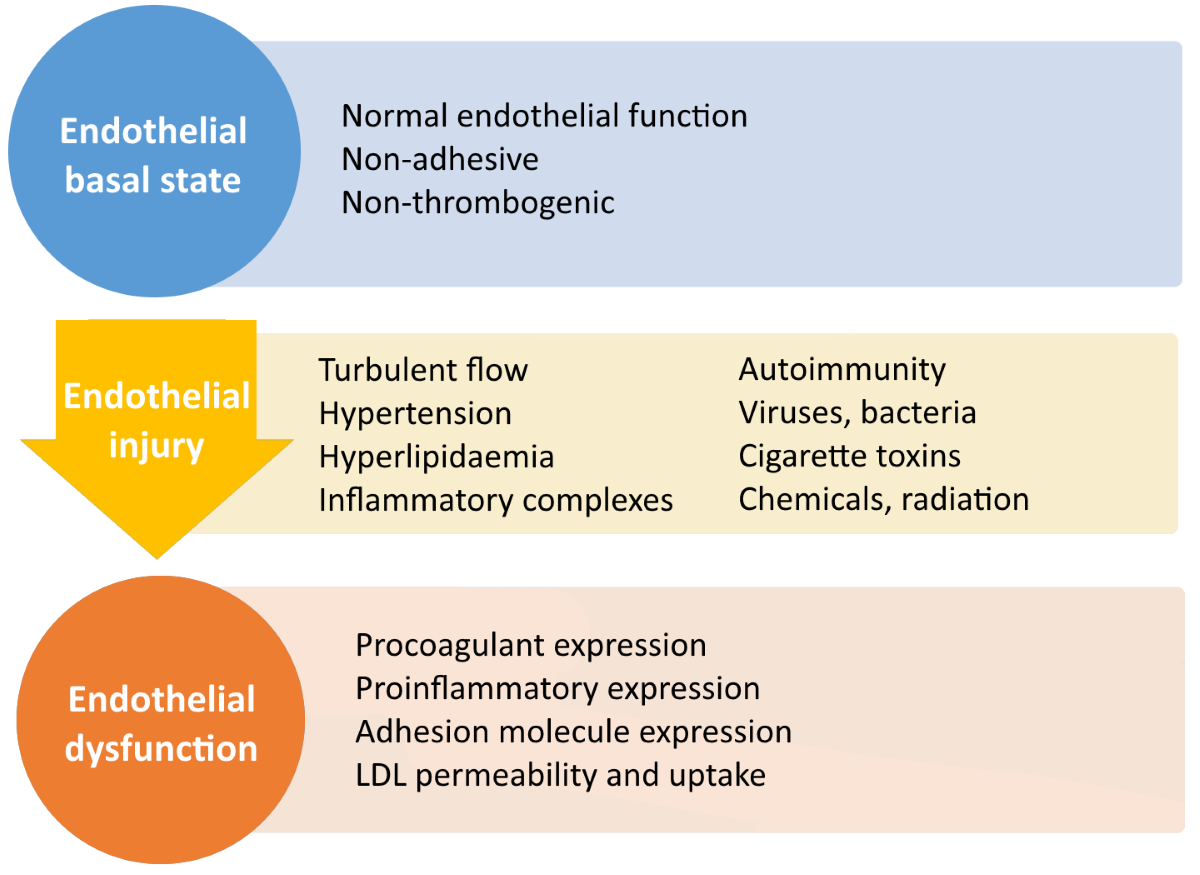
Endothelial Injury
Endothelial Dysfunction
- Endothelium becomes 'sticky' with adhesion molecules
- Platelet adhesion → thrombogenicity
- Monocyte infiltration
- Increased LDL permeability and uptake
Endothelial Dysfunction
Proliferation, Oxidation, Engulfment
- Smooth muscle cells proliferate
- in response to growth factors
- from platelets and macrophages
- Accumulated LDL is oxidised
- by free radicals released from macrophages and stressed endothelial cells
- oxLDL stimulates release of growth factors, cytokines, chemokines and recruits monocytes
- oxLDL is cytotoxic to endothelial and smooth muscle cells
- Macrophages and smooth muscle cells engulf oxLDL
- become foam cells
Proliferation, Engulfment
Fibrous Cap, Necrotic Core
- Continued smooth muscle proliferation:
- extracellular matrix generation
- collagen secretion
- fibrous cap formation
- Increasing size:
- necrosis of thickening intima → necrotic core
- stimulation of neovascularisation
Fibrous Cap, Necrotic Core
Overview: Response to Injury Hypothesis
Risk Factors
| Constitutional | genetics family history age, gender |
| Modifiable | hyperlipidaemia hypertension diabetes smoking diet |
Risk factors are roughly multiplicative
Age, Gender
- Age: presentations in middle age and beyond
- Male gender: pre-menopausal women protected, risk equalises after menopause
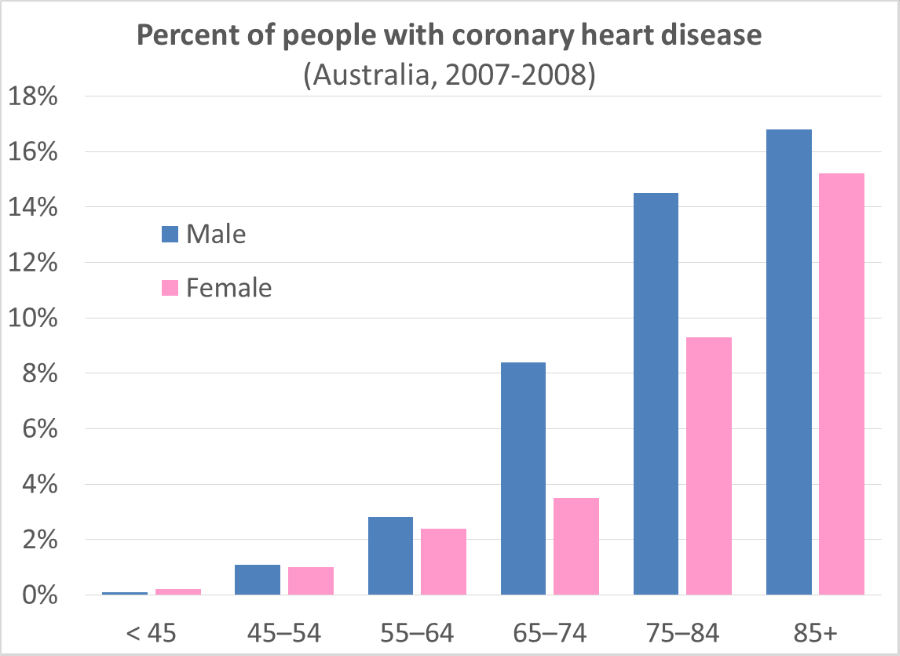
Data: AIHW
Genetics
-
some Mendelial disorders
-
(e.g. familial hypercholesterolaemia)
-
mostly polygenic traits and polymorphisms
Family History
-
especially 1st degree heart disease <50 y/o
Hypertension
- Systolic >140 mmHg
-
Diastolic >90 mmHg
-
Includes 25% of population
Hypercholesterolaemia
-
Risk: LDL
- distributes lipids to tissues
- Protective: HDL
- extracts lipids from atheromas
- transports to liver for excretion

Lifestyle
-
Smoking
- Obesity
-
Little exercise
Diet
- Main effect: lipid profile alteration
- Bad: cholesterol, saturated fats
- Good: omega-3 fatty acids, polyunsaturated fats



Diabetes Mellitus
- Raised cholesterol levels
- Increased risk of stroke and MI
- Particularly increased risk of
atherosclerosis-associated gangrene

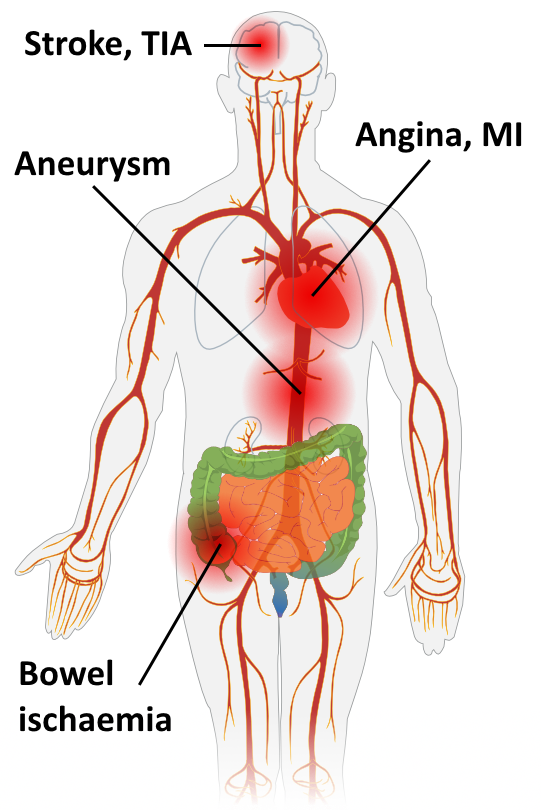
Acute Complications
- Weaken wall → aneurysms
- Rupture → thrombosis, thromboembolism
- Obstruct lumen → stenosis
-
Stroke
, transient ischaemic attacks (
TIAs
)
-
Angina
,
MI
-
Bowel ischaemia
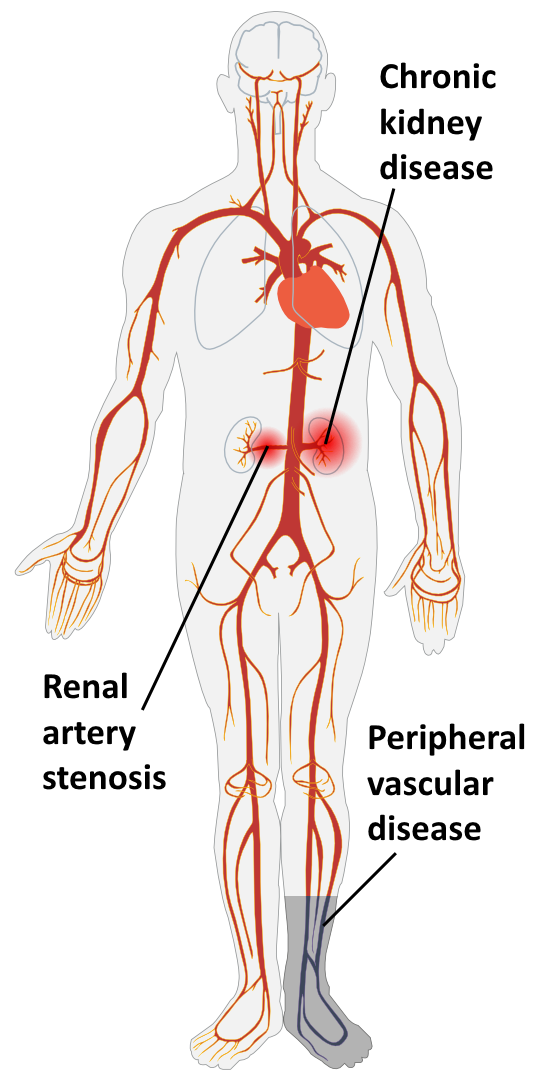
Chronic Complications
-
Peripheral vascular disease
- especially diabetics and elderly
- pallor, cyanosis, pain
- intermittent claudication
- ulceration, gangrene
- Renal artery stenosis
- Chronic kidney disease
Fatty Streak
- Fatty streaks form almost universally as young as childhood
- Especially at branch points and turbulent zones
- No clinical significance, don't necessarily progress
Atheroma
- Risk factors accelerate progression
- Protrusion into lumen, wall remodelling to compensate
- Decompensation of remodelling >50% diameter → stenosis
Complicated Plaque
- Surface ulceration, fissuring
- Haemorrhage
- Aneurysm
- Rupture
- thomobosis and occulusion
- thomboembolism
See page for author [GFDL or CC-BY-SA-3.0], via Wikimedia Commons
Complicated Plaque
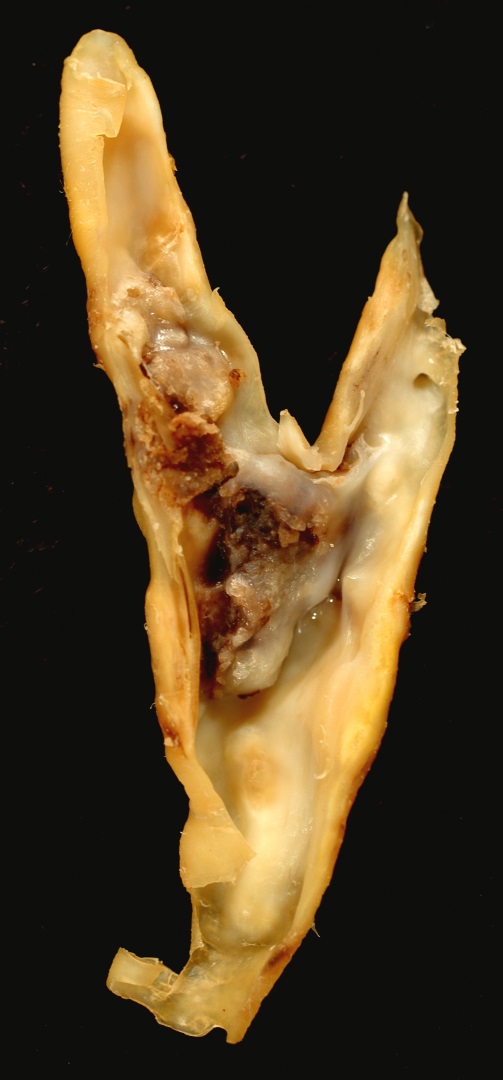
Ed Uthman [CC-BY-2.0], via Wikimedia Commons
Treatment
- Main treatment is to modify risk factors for progression
- Lifestyle: diet, exercise, weight loss, smoking
- Hypertension: anti-hypertensives
- Hypercholesterolaemia: statins, fibrates
- Diabetes control
- Reduce risk of thrombosis: aspirin
- Surgical: stents, bypasses

