
Definition
-
Immune response to dietary gluten
- Damage to proximal small intestine epithelium
-
Malabsorption features
- Responds to gluten-free diet
Other Names
- Coeliac sprue
- Gluten-sensitive enteropathy

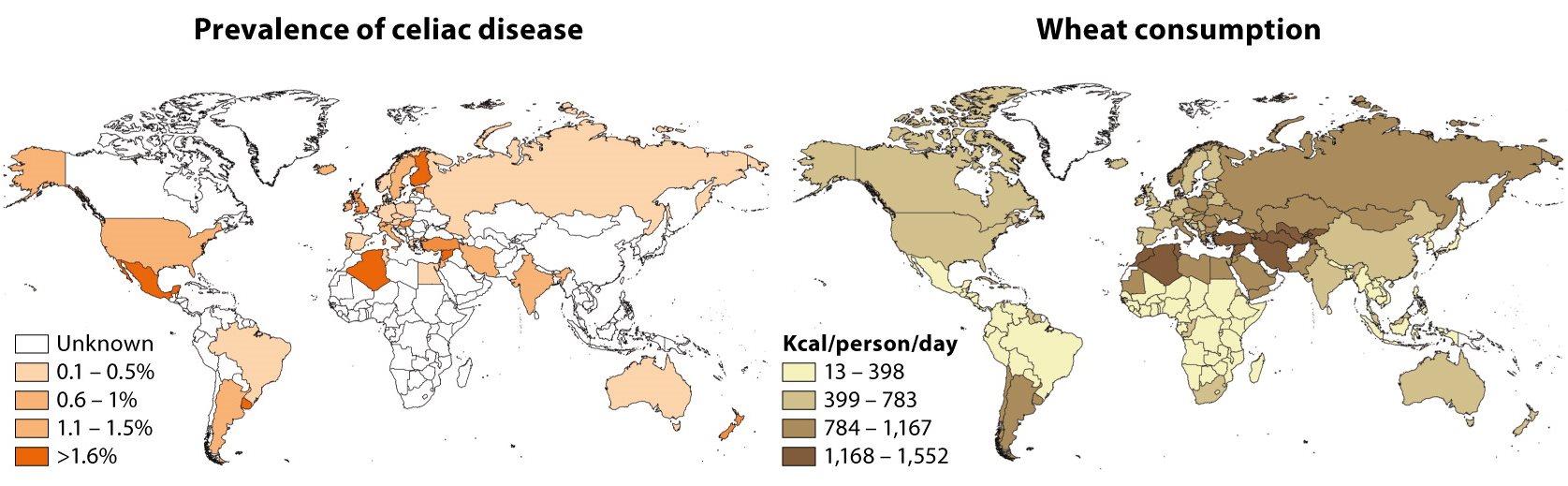
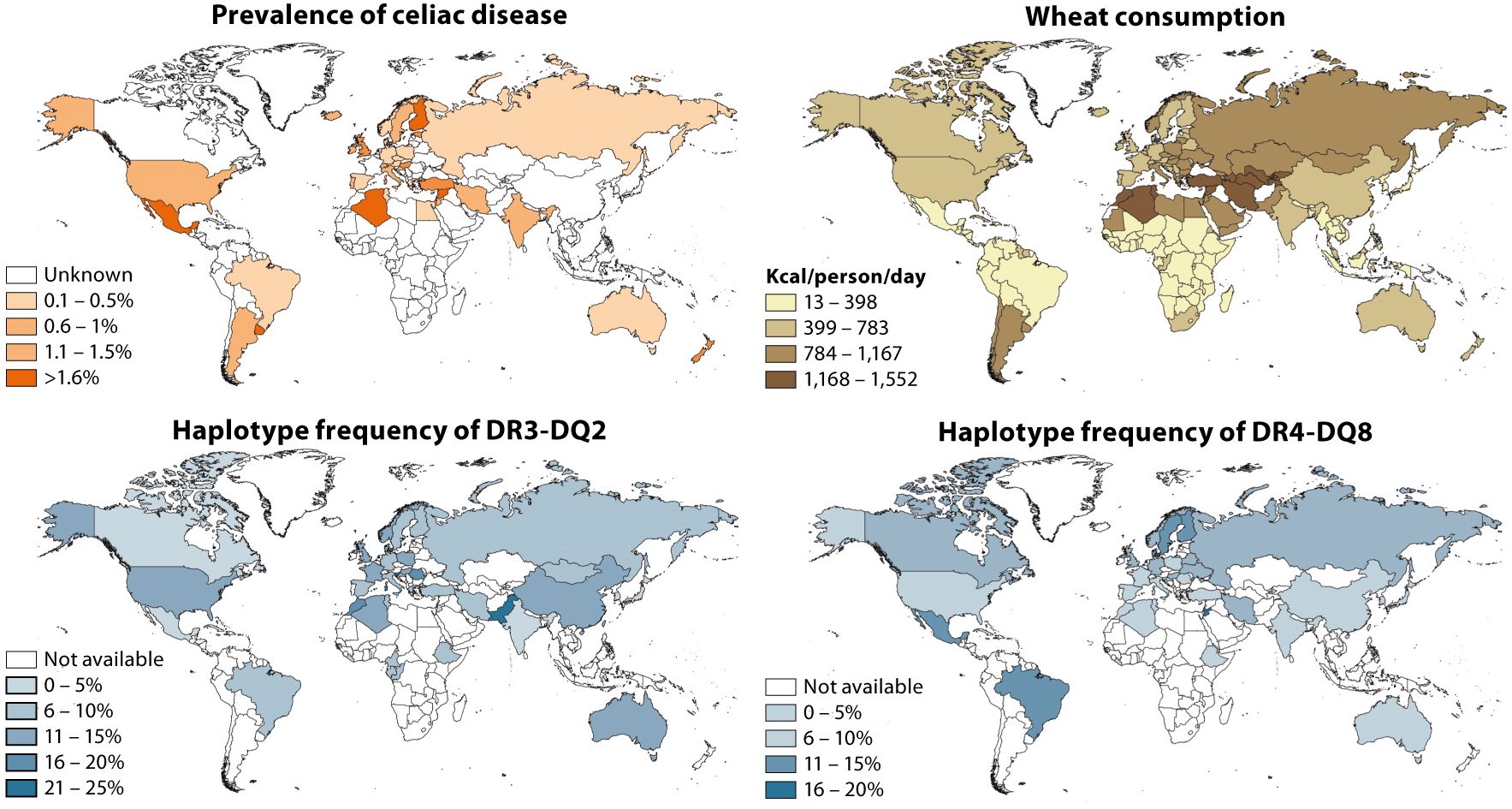
Prevalence
-
0.5 to 1% among those of White European ancestry
- Most commonly 30-60y with peaks in infancy and in 50s
Morbidity
Patient perceptions
| Complaint | % reporting |
|---|---|
| Reduced enjoyment of food | 68% |
| Food costs >£10 per week extra | 46% |
| Food costs a problem | 21% |
| Doing enjoyable things less often | 54% |
| Regret not being diagnosed earlier | 66% |
Mortality
-
Mainly in undiagnosed and untreated
-
Most mortality from malignancies
-
Long-term survival when properly treated


Data: Violata, M. et al., 2012
Pathogenesis
- Immune-mediated reaction to gluten in intestine
- Most people have no problem with gluten
- Thus disease attributable mainly to host factors
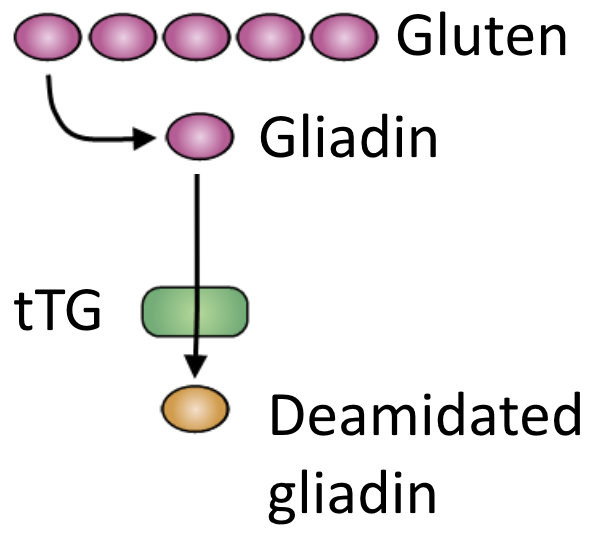
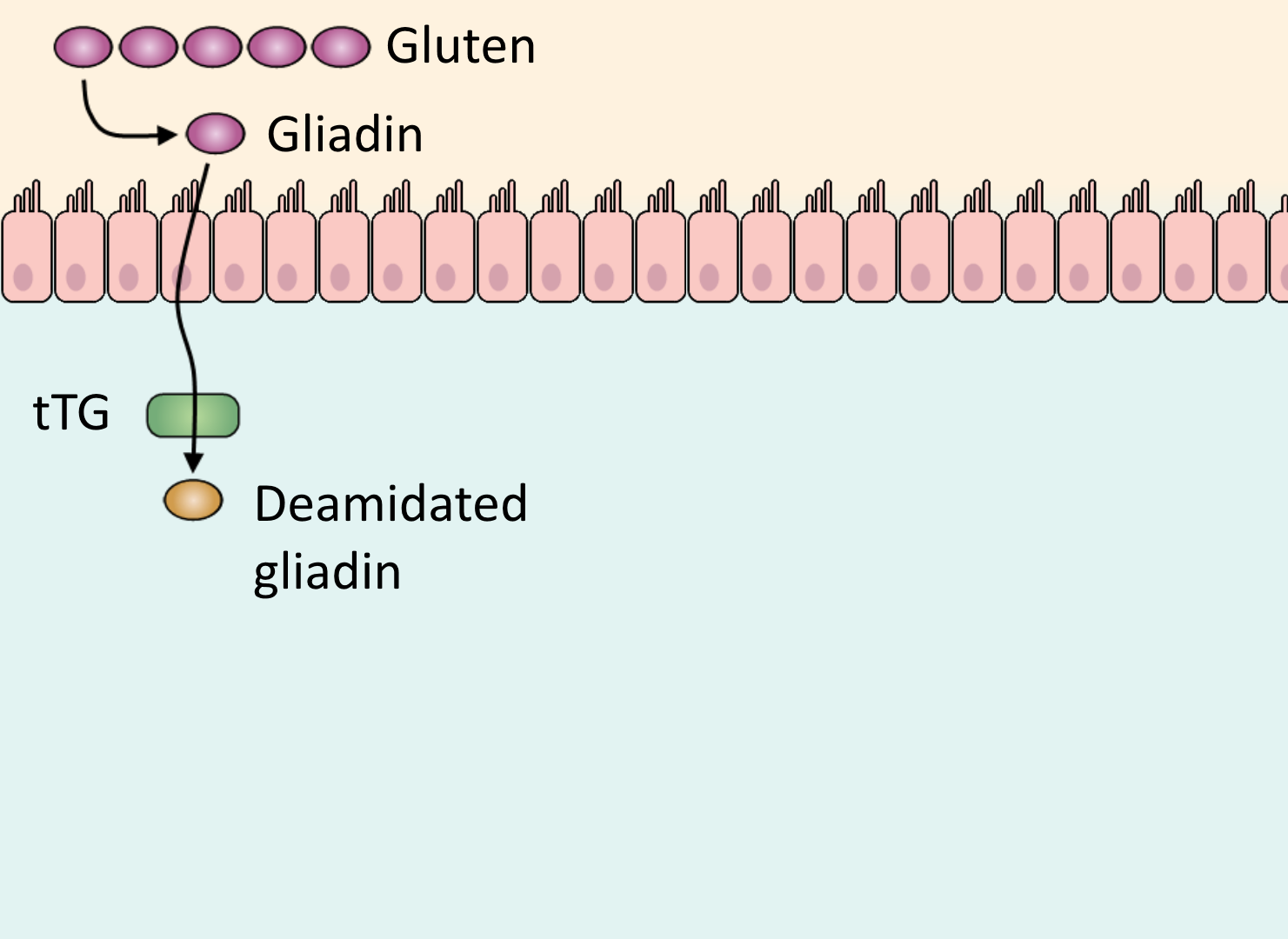
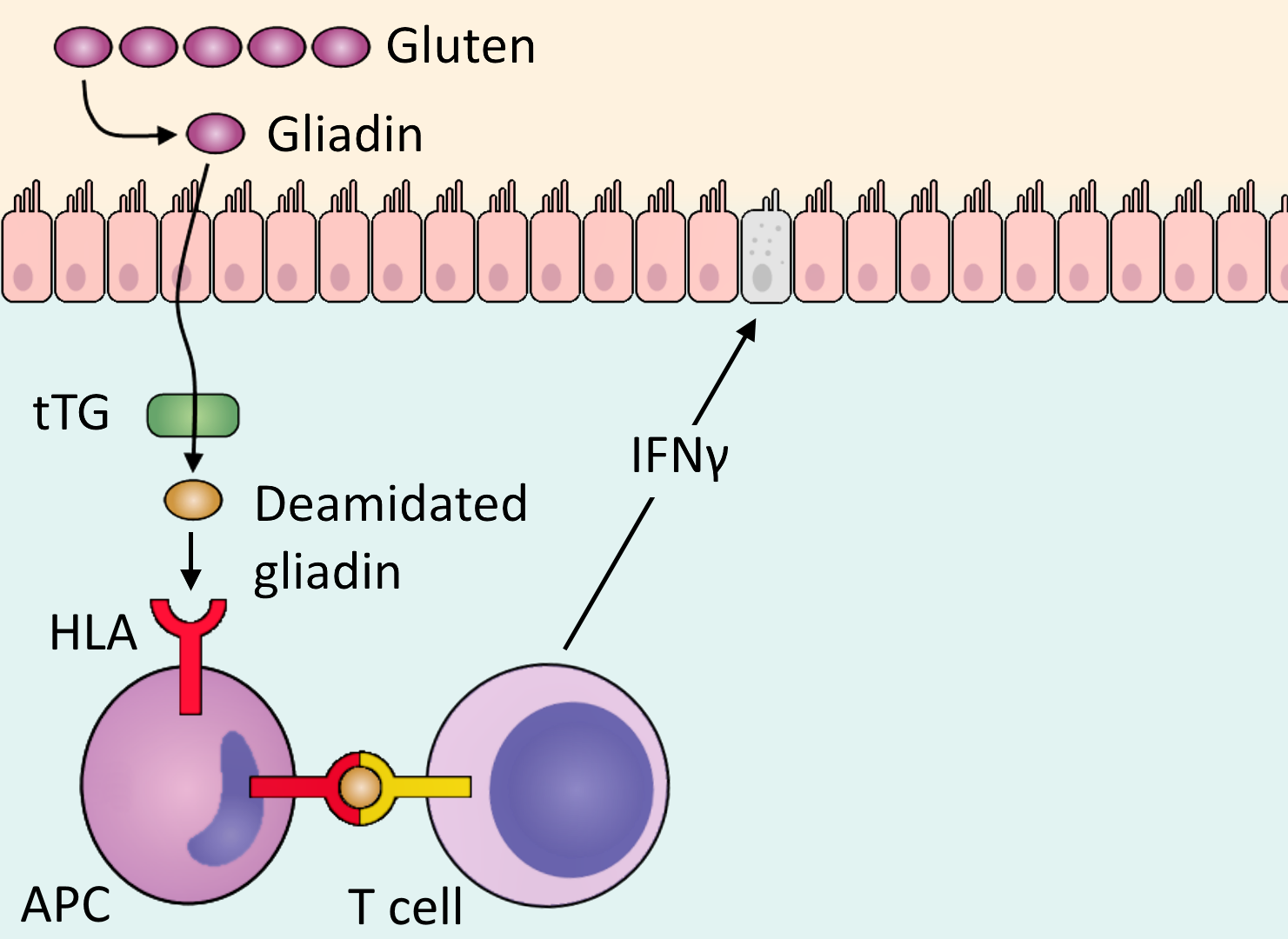
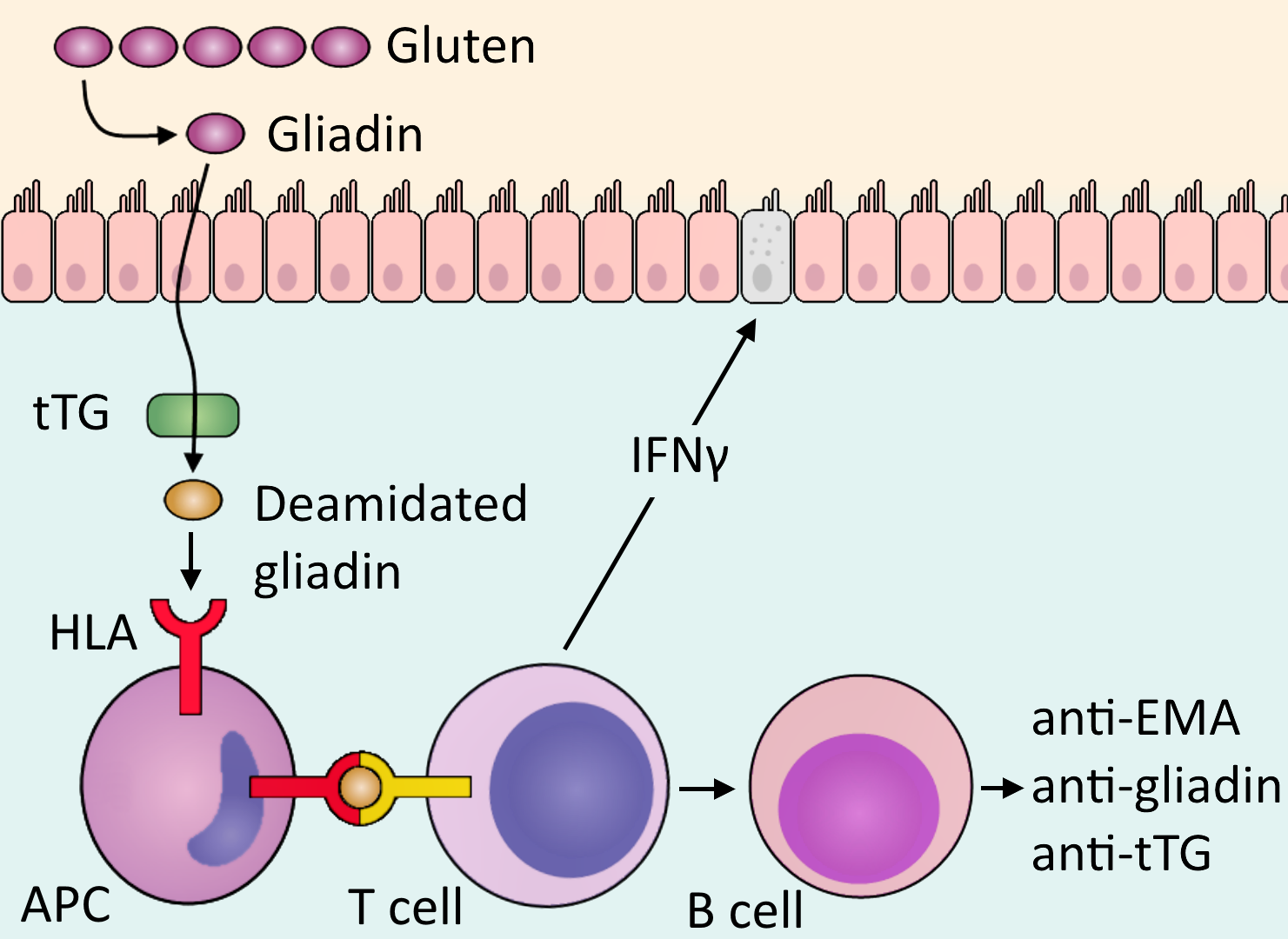
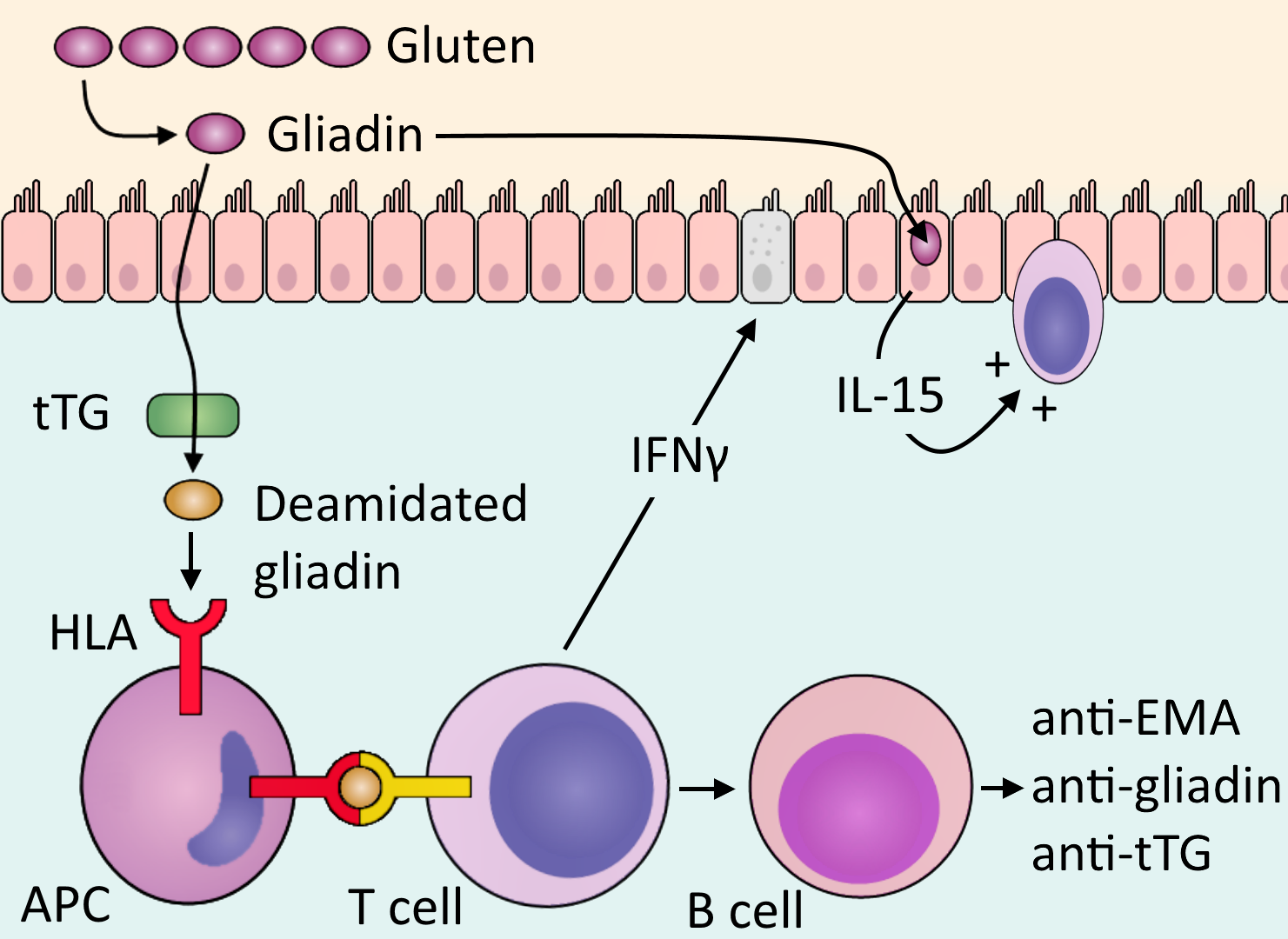
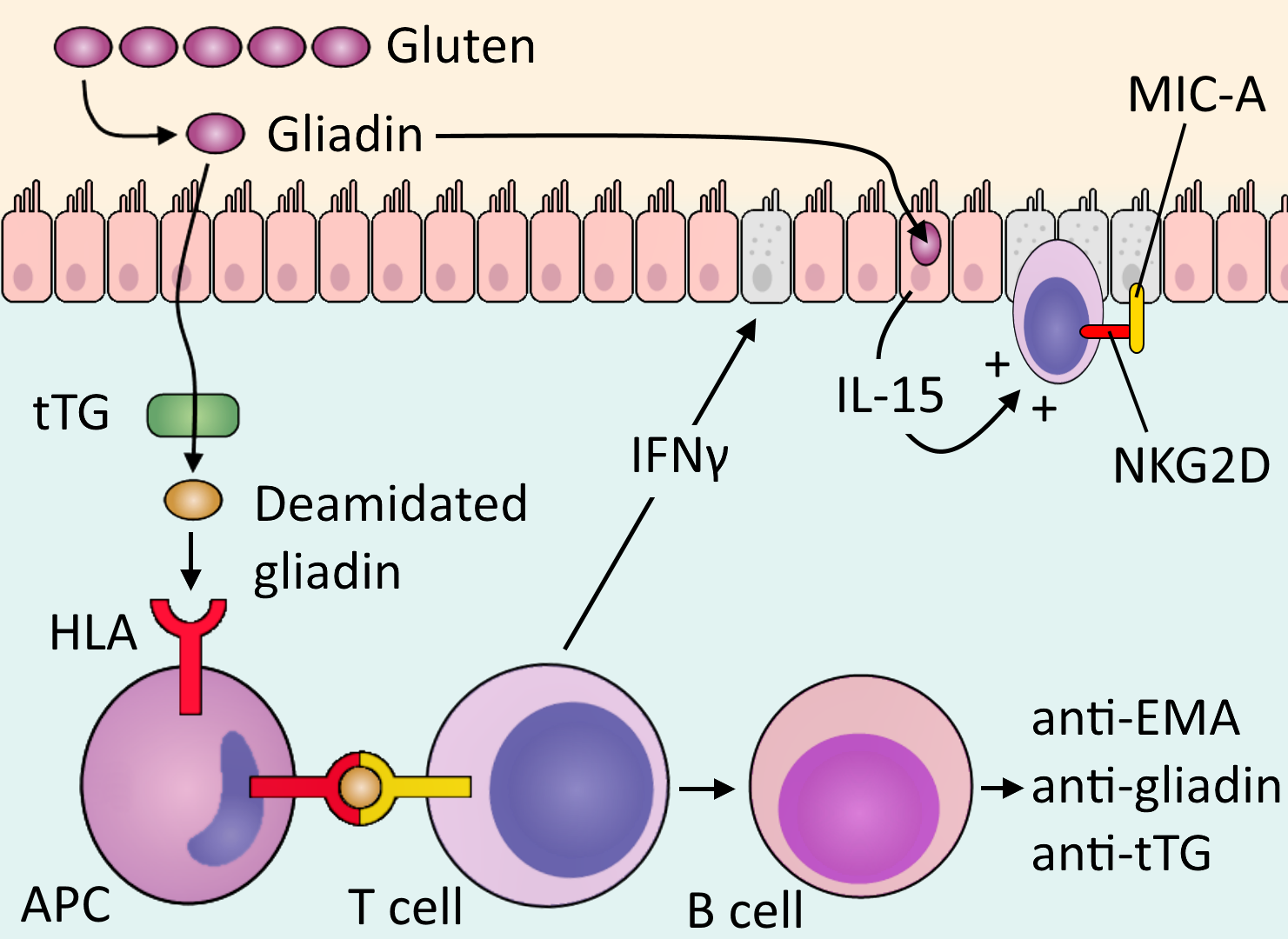
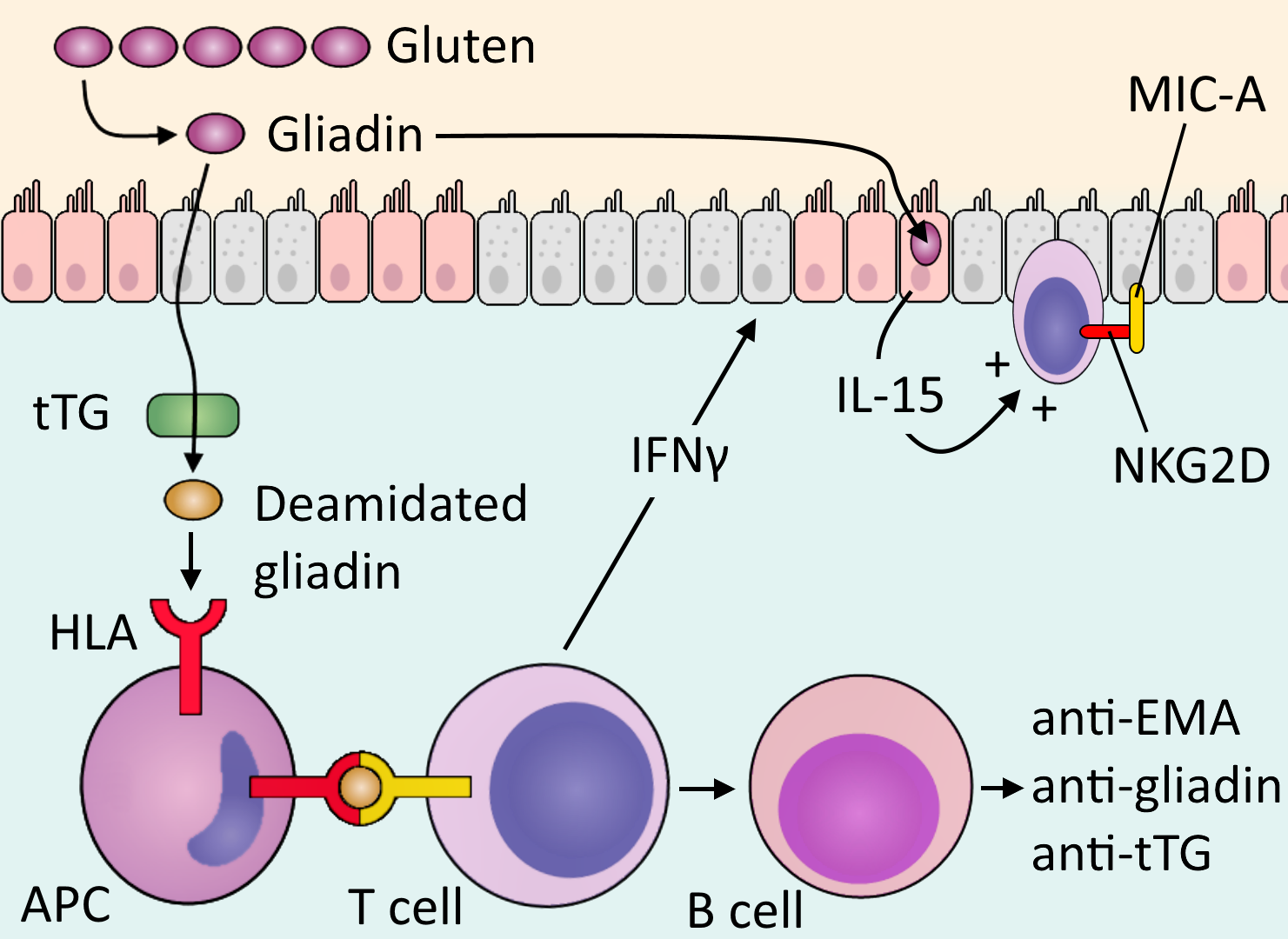
Digestion, Ingestion
- Gluten is ingested in cereal grains (wheat, rye, barley).
- Gluten is digested by intestinal enzymes to amino acids and peptides.
- A peptide, gliadin, remains, which cannot be degraded by regular enzymes
- Gliadin is instead deamidated (has an amide group removed) by tissue transglutaminase (tTG).
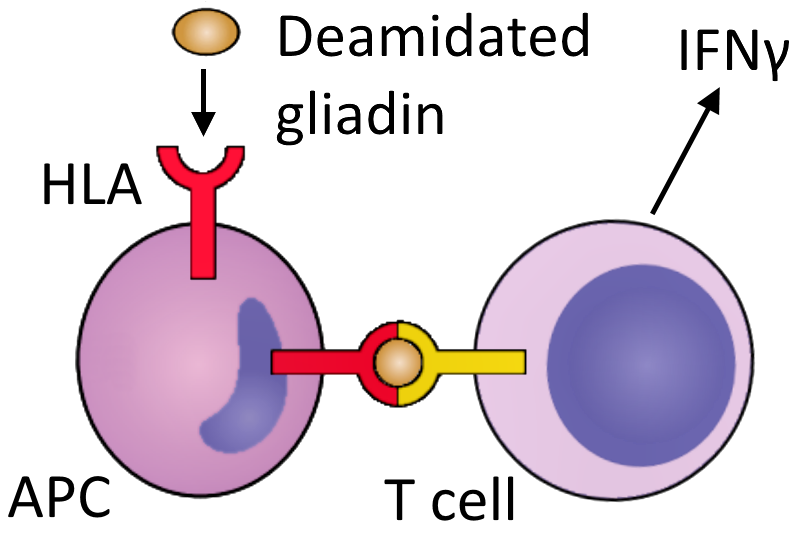
APC Presentation, T cell response
-
Deamidated gliadin interacts with HLA DQ2 or HLA DQ8 on antigen presenting cells (APCs).
- Deamidated gliadin is presented to CD4 T cells.
- CD4 T cells produce cytokines (such as IFNγ) which cause tissue damage.
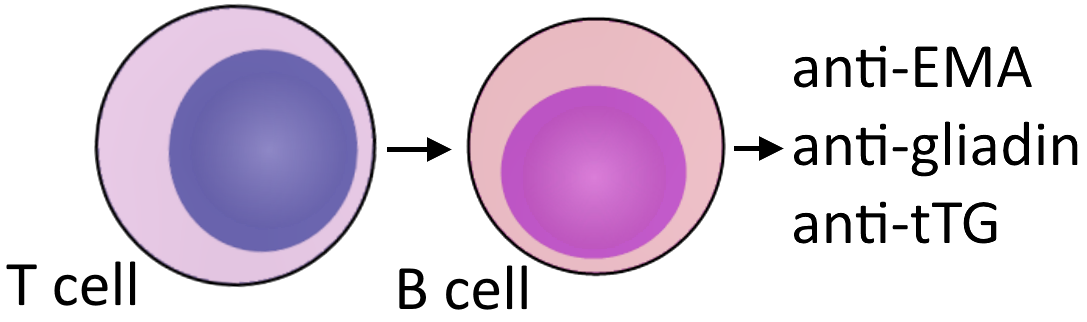
B cell response
- T cells also elicit a B cell response.
- B cells produce the antibodies:
- Anti-tissue transglutaminase (anti-tTG)
- Anti-deamidated gliadin
- Anti-endomysial antibody (anti-EMA)
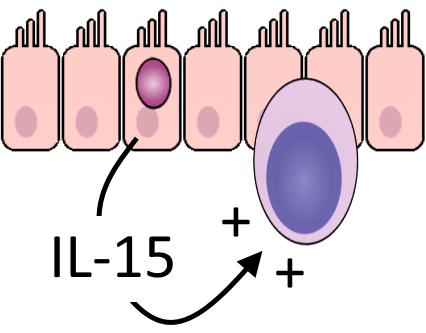
IL-15, intraepithelial lymphocytes
- Gliadin also induces IL-15 production from enterocytes.
- IL-15 activates and upregulates intraepithelial CD8 lymphocytes.
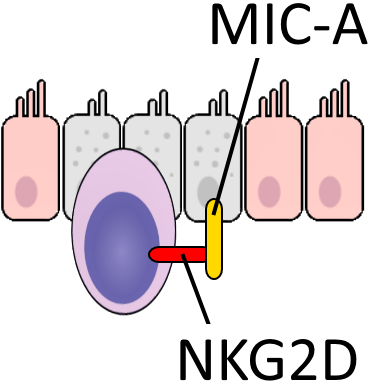
MIC-A, NKG2D
-
Various stressors causes
MIC-A
to be expressed on enterocytes.
- Intraepithelial lymphocytes receive MIC-A via NKG2D in a cytotoxic interaction, killing enterocytes.
Progression
- Tissue damage progresses with villous atrophy and loss of surface area.
- Damage allows increased movement of gliadin across the epithelium, amplifying disease.
- An increased rate of mitosis is seen with reduced enterocyte differentiation and function.
- Tissue damage, loss of surface area, and reduced function result in malabsorption.
Clinical features
- Many atypical presentations, often an incidental finding
- Presentations most commonly 30-60y, but any age
- Peaks in infancy and 50s
- No gender difference, but 2-3x more women detected
- menstrual blood loss potentiates anaemia

Disease associations
- Immune diseases and atopy:
- Diabetes mellitus type 1
- Thyroiditis
- Sjögren syndrome
- Other diseases:
- Epilepsy
- IgA nephropathy
- Down syndrome
- Turner syndrome
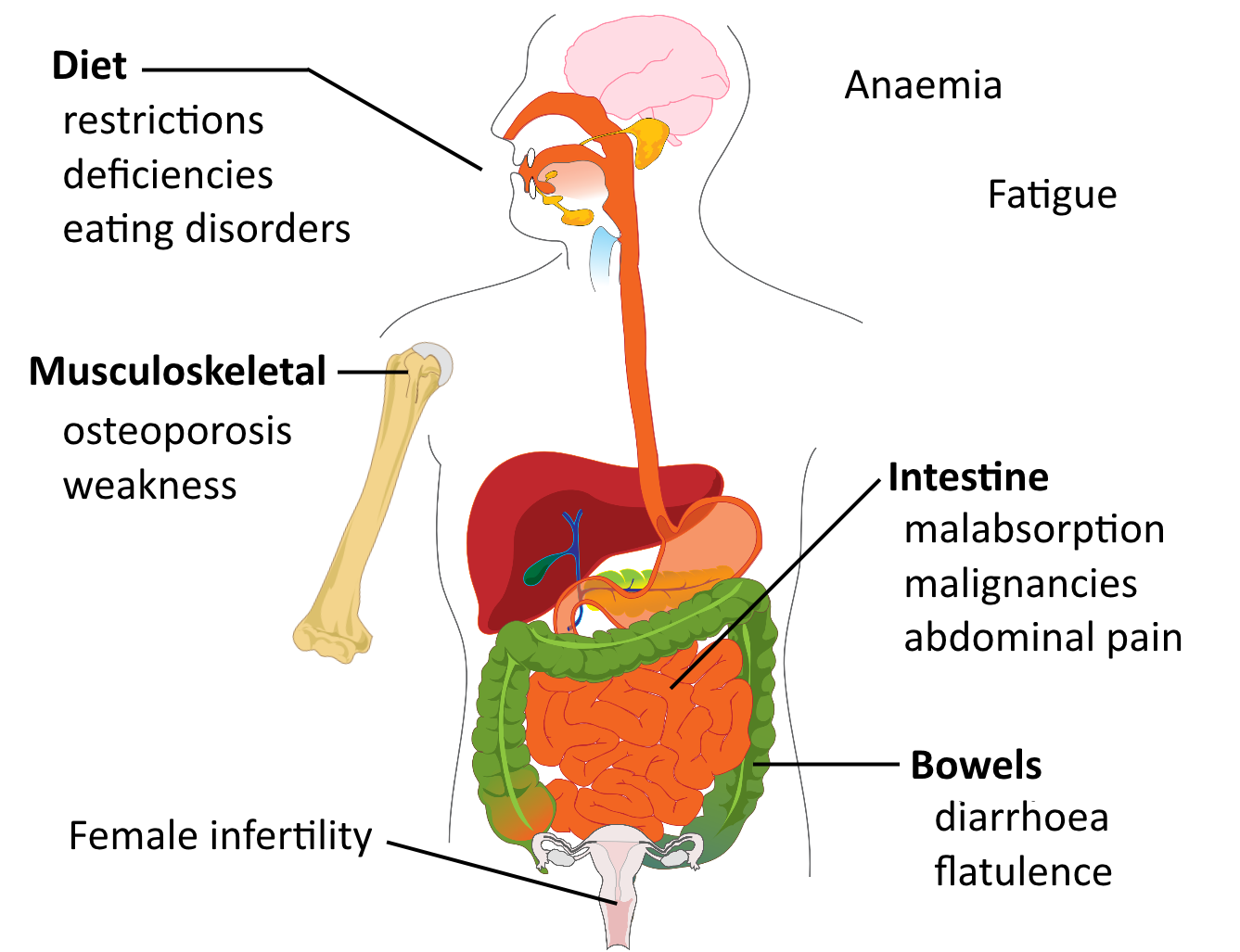
Symptoms
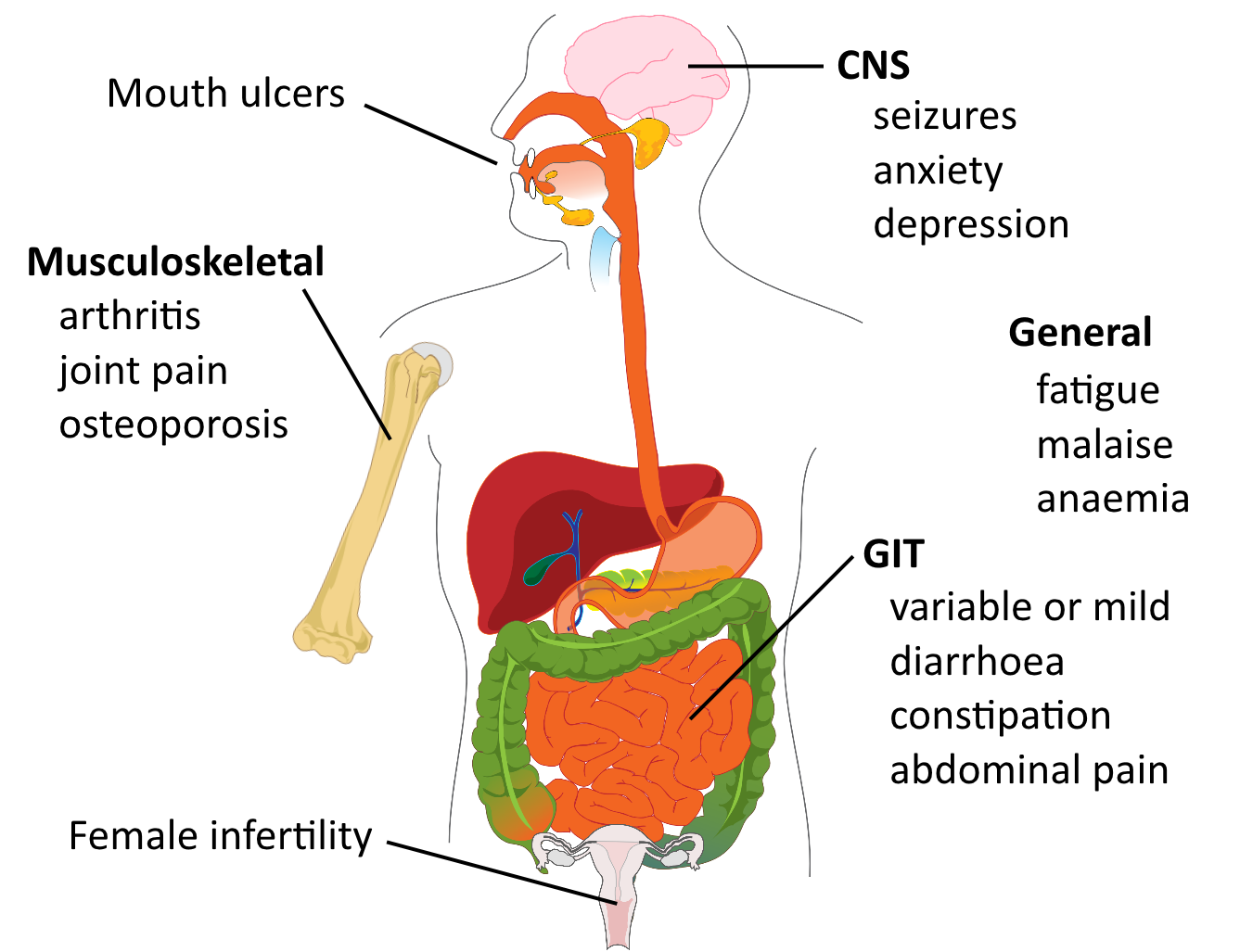
Malabsorption-related symptoms
| Manifestation | Malabsorbed nutrient |
|---|---|
| Steatorrhoea | Fats |
| Diarrhoea | Fats, carbohydrates |
| Manifestation | Deficiency |
|---|---|
| Weight loss, wasting | Fats, proteins, carbs |
| Anaemia | Iron, vit B12, folic acid |
| Paraesthesia, tetany | Calcium, vit D |
| Osteoporosis, arthritis | Calcium, vit D |
| Bleeding, bruising | Vit K |
| Oedema | Protein |
Dermatitis herpetiformis
- 10% of patients
- Similar appearance to herpes
- Itchy papulovesicular rash

BallenaBlanca [CC-BY-SA-3.0], via Wikimedia Commons
Paediatric
- Classical:
- 6-24 months
- Irritability
- Abdominal distension, diarrhoea
- Anorexia, weight loss, failure to thrive
- Muscle wasting
- Non-classical:
- Older ages
- Abdominal pain, nausea, vomiting
- Bloating, constipation
Signs
- Few and non-specific
- Anaemia
- tachycardia
- pallor
- Bruising (vit K deficiency)
- Hyperactive bowel sounds
- Neurological signs
- Oedema (severe cases)
HLA DQ2, HLA DQ8
- 95% of patients have at least one
- accounts for 50% of genetic component
Other risk factors
- Other immune system polymorphisms:
- e.g. IL-2, IL-21
- Other ill-defined genetic components:
- 10-15% of 1st degree relatives (may be clinically silent)
- 70% monozygotic twin concordance
- Breast feeding and gluten introduction ages significant
- Infant rotavirus infection
Serology
- Conduct non-invasive serology before biopsy
- Also for dietary compliance monitoring
- 2.5% of coeliac patients have IgA deficiency
- Verify normal levels
- Investigate IgG if IgA deficient
| IgA anti-tTG | + sensitive |
| IgA or IgG anti-demanidated gliadin | + sensitive |
| Anti-EMA | ++ specific, - sensitive |
| HLA DQ2/DQ8 | cannot confirm diagnosis helps exclude diagnosis if negative |
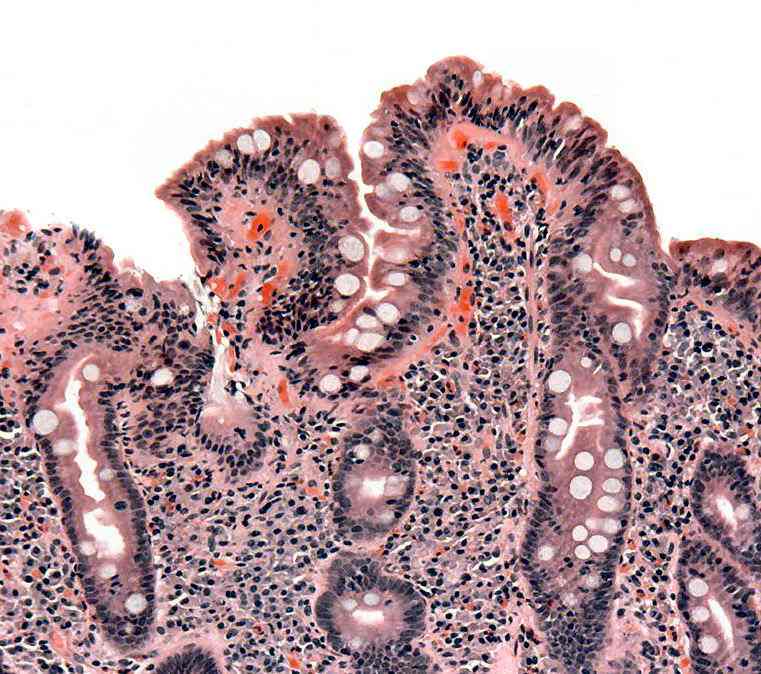
Biopsy
- Small bowel endoscopic biopsy
- 'Gold standard', but not always necessary in clear-cut cases with serology
-
Not specific, other causes, need serology also
- Histology:
- Sub-total villous atrophy
- Increase in lamina propria, lymphocytes, plasma cells, mast cells and eosinophils
Acute complications
- Mostly rare
- Anecdotal intestinal obstructions and perforations
-
Coeliac crisis
- acute, fulminant worsening of symptoms
- often with a gluten challenge
- hypoproteinaemia, oedema
- severe diarrhoea
- dehydration, electrolyte imbalance
- metabolic acidosis
- hospitalisation, fluid replacement, corticosteroids
Chronic complications
- Refractory coeliac disease (RCD)
- improvement with diet, then loss of response
- increased complications (malignancy), poor prognosis
- Malignancy risk
- Enteropathy-assoc. T cell lymphoma
- Small intestinal adenocarcinoma
Chronic complications
- Ulcerative jejunitis
- Anaemia
- Female infertility
- Osteoporosis (even when on strict diet)
- Malnutrition, cachexia
- Paraesthesia, ataxia, muscle weakness
- Splenic atrophy
- need pneumococcal vaccinations
Treated
- Initial supplementation of mineral and vitamin body stores
- Gluten-free diet
- Improvement in symptoms within days/weeks
- Improvement in morphology after months
- Long-term survival, unrelated mortality
-
Challenging and costly to maintain
- Long-term risk of small intestinal and oesophageal malignancy
Untreated
-
Poor compliance relatively common
- Elaboration of malabsorption features
- Severe diarrhoea
- dehydration, electrolyte imbalances
- Osteoporosis
- Malignancy
-
Neurological, psychiatric complications
- Children
- growth retardation
- short stature
- Pregnancy
- miscarriage
- congenital malformations
