Definition
Cancer of the colon or rectum
| Type | Frequency | Cellular origin |
|---|---|---|
| Adenocarcinoma | 95% | Glandular epithelium |
| Lymphoma | 1% | Extranodal lymphatic system |
| Carcinoid | 0.5% | Neuroendocrine cells |
| Sarcoma | 0.3% | Blood vessels, muscle, connective tissue |
| Squamous cell | rare | Squamous cells |
| Stromal | rare | Interstitial cell of Cajal |
Adenocarcinoma
-
By far the most common
-
"Colorectal adenocarcinoma"
used interchangeably with
"colorectal cancer"
Lifetime Incidence
- 1 in 20 will develop in lifetime
-
1 in 50 will die from in lifetime

Prevalence
- 3rd most common cancer worldwide
(10% of total cancers)
- Steadily increasing incidence
- ↑ 30% among males since 1975
- Ageing population?
- Westernised diet?
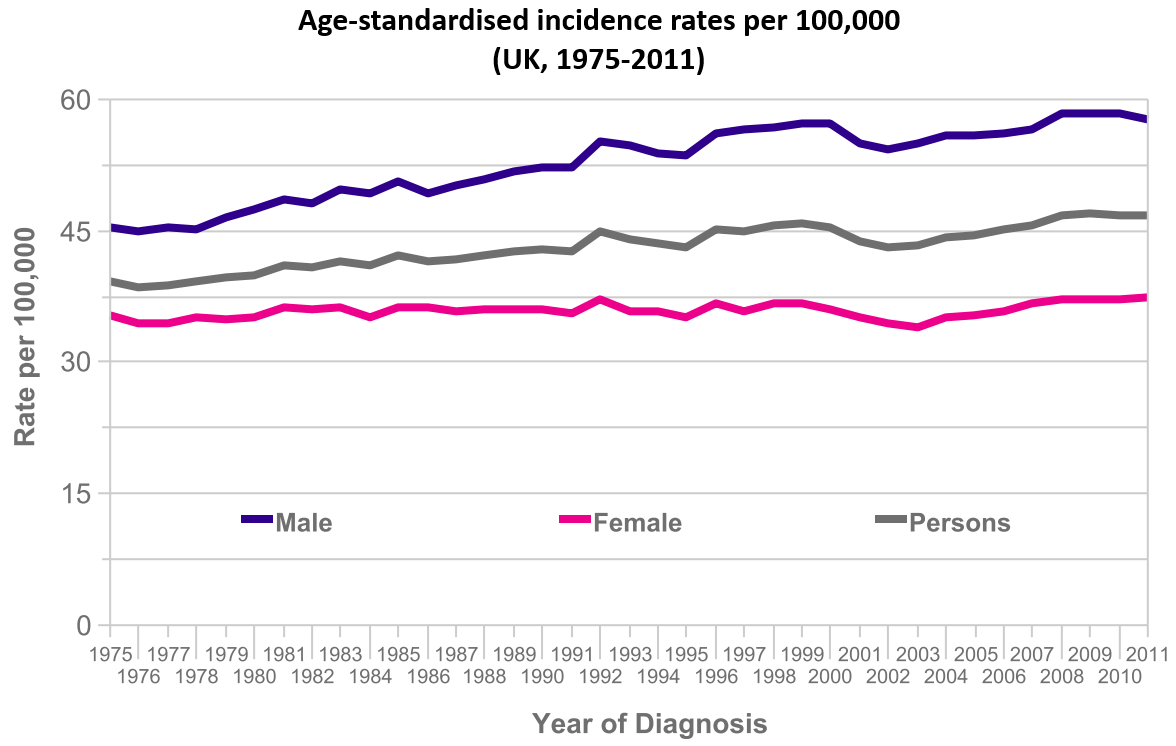
Ref: Cancer Research UK
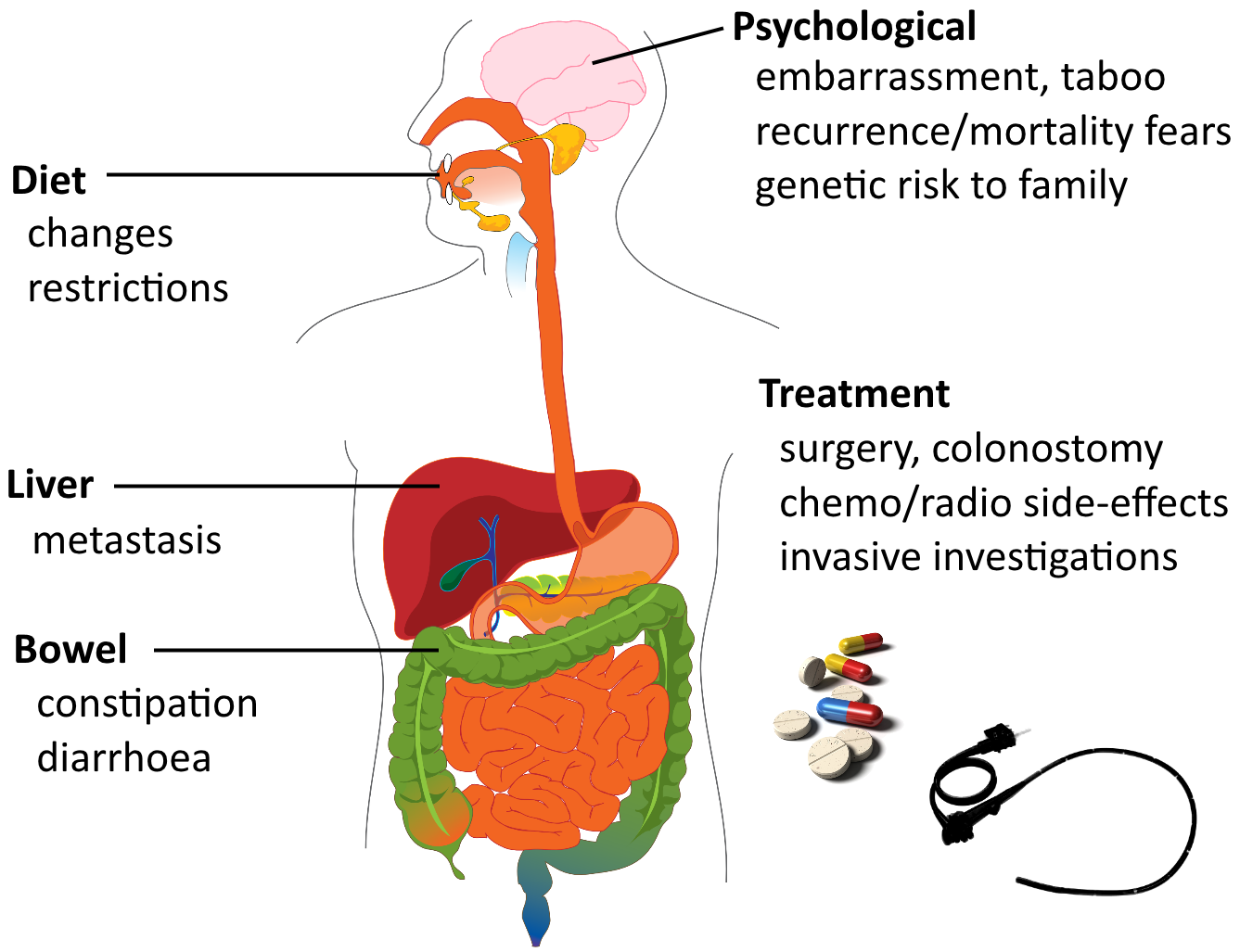
Morbidity
Mortality
- 40% overall
- 2nd-3rd most responsible for cancer-related mortality
Data: O'Connell et al.
Cost
Ireland, 2008
(Ref: Tilson et al.)
-
Average healthcare cost per case = ~€40,000
-
More for rectal cancers
-
More for advanced stages
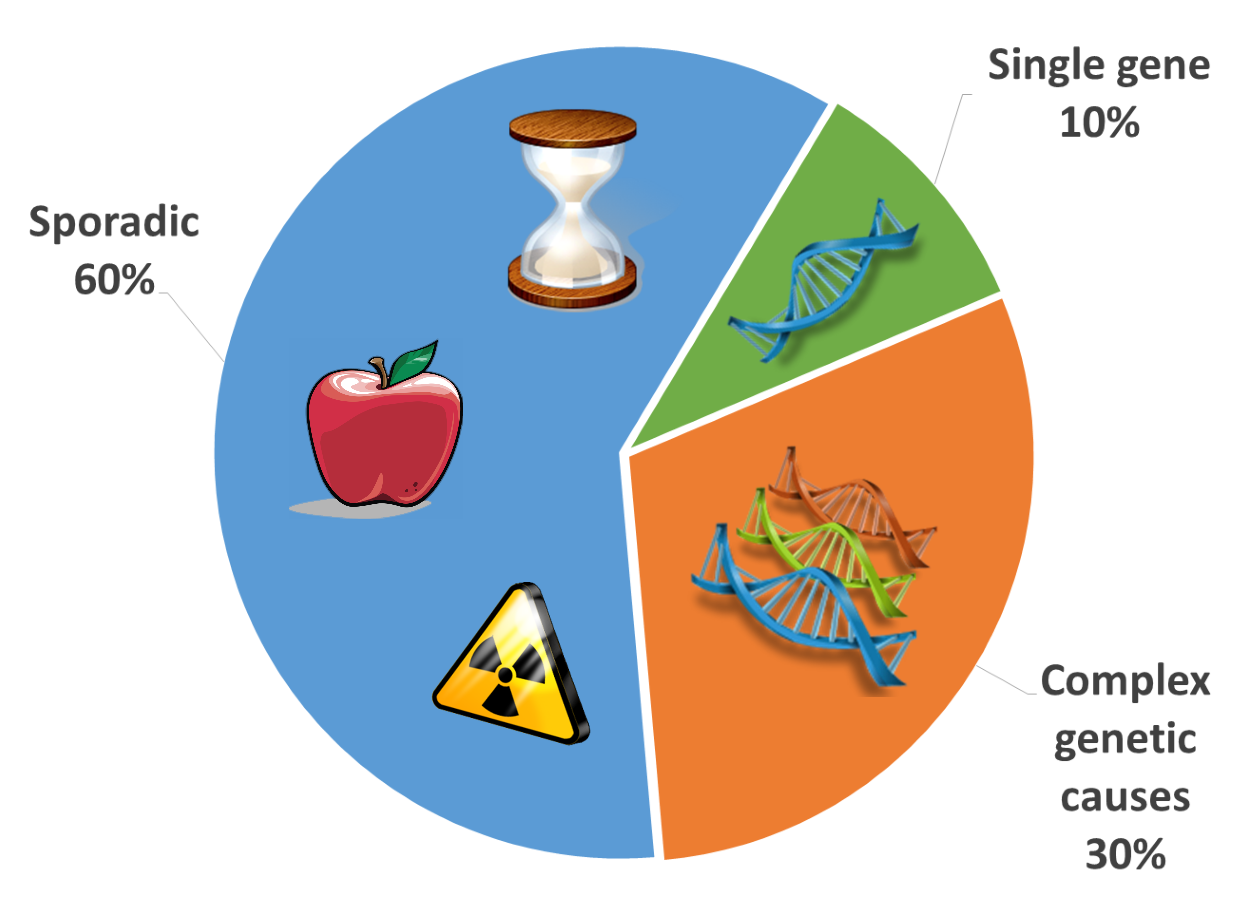
Pathogenesis
- 5-10% single gene disorders
- HNPCC (MLH1, MSH2 genes)
- FAP (APC gene)
- 30% complex genetic causes
- 60% sporadic
- age-associated
- Western diet
- chronic inflammation
- abdominal radiation
- immunosuppression
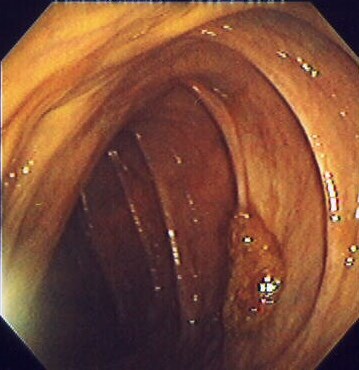
Polyps
Small growths from mucous membranes
Kd4ttc [CC-BY-2.5], via Wikimedia Commons

Pedunculated polyp

Ed Uthman [Public domain], via Wikimedia Commons
Polyps
- Neoplastic polyps
- Adenomatous polyps (adenomas)
- 10% of all polyps
- Potential for malignant change, but most do not
-
Non-neoplastic polyps
- Inflammatory, hamartomatous, hyperplastic
- 90% of all polyps
- Generally no malignant change
- A sign of greater risk of adenoma (carcinoma)

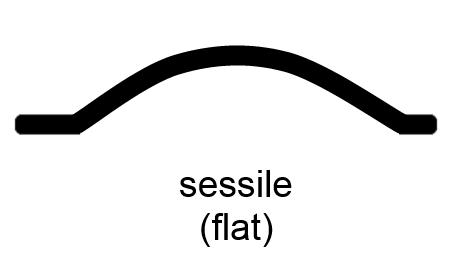
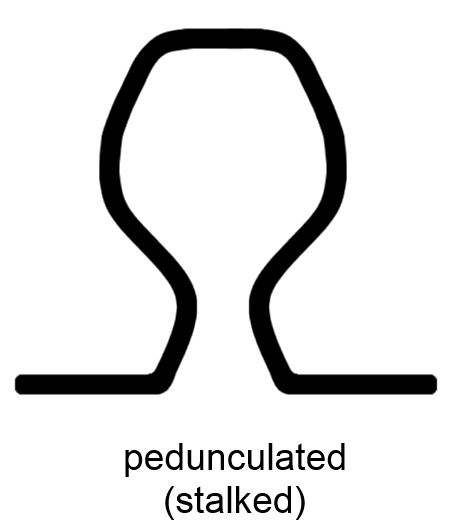
Adenomas
- 0.3 to 10 cm diameter
- Velvety, raspberry-like texture of irregular epithelium
- Sessile or pedunculated

Ed Uthman [CC-BY-SA-2.0], via Wikimedia Commons
Adenoma Architectures
- Tubular: small, peduncular, tubular glands
- Tubulovillous
- Villous: larger, sessile, villous surface
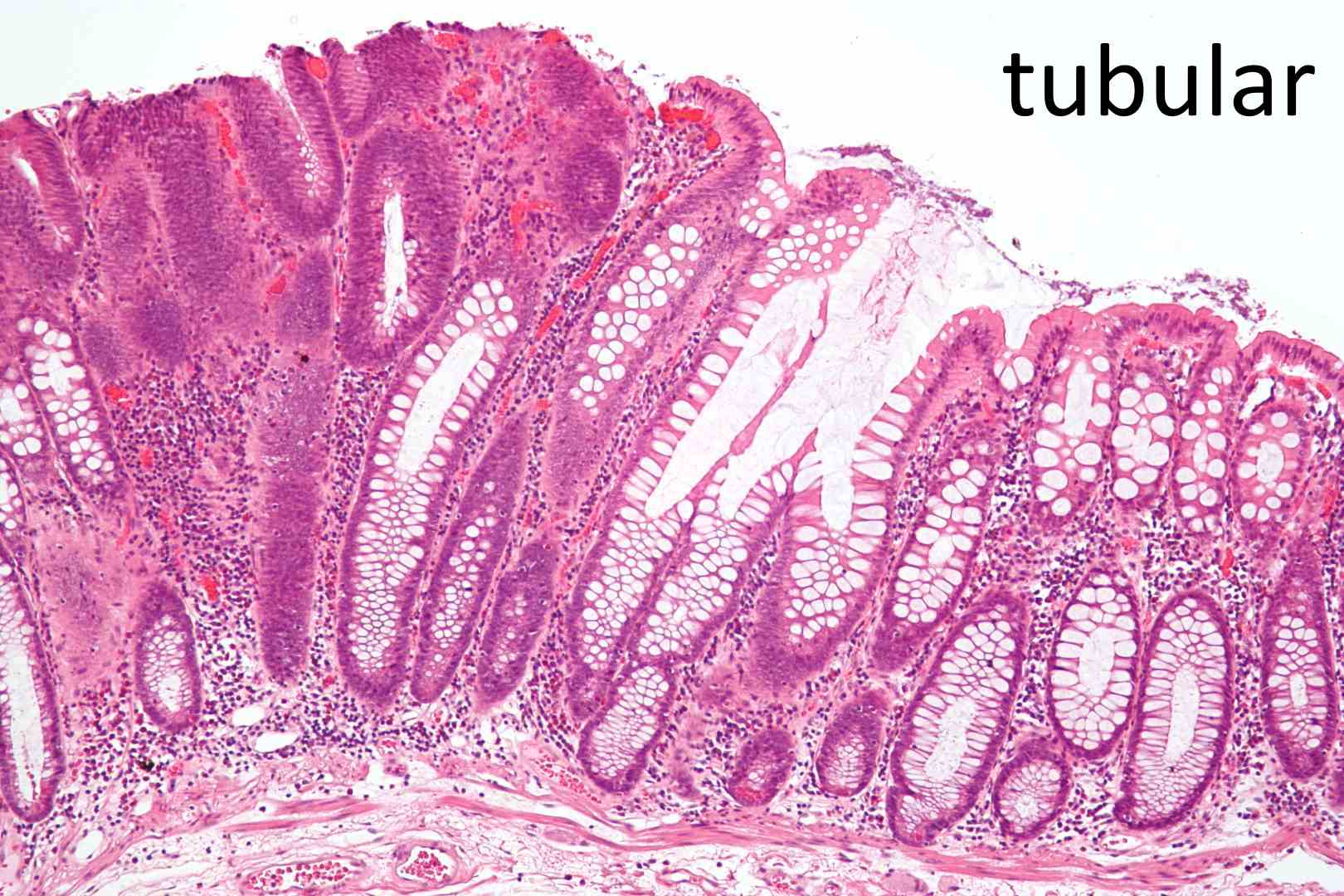
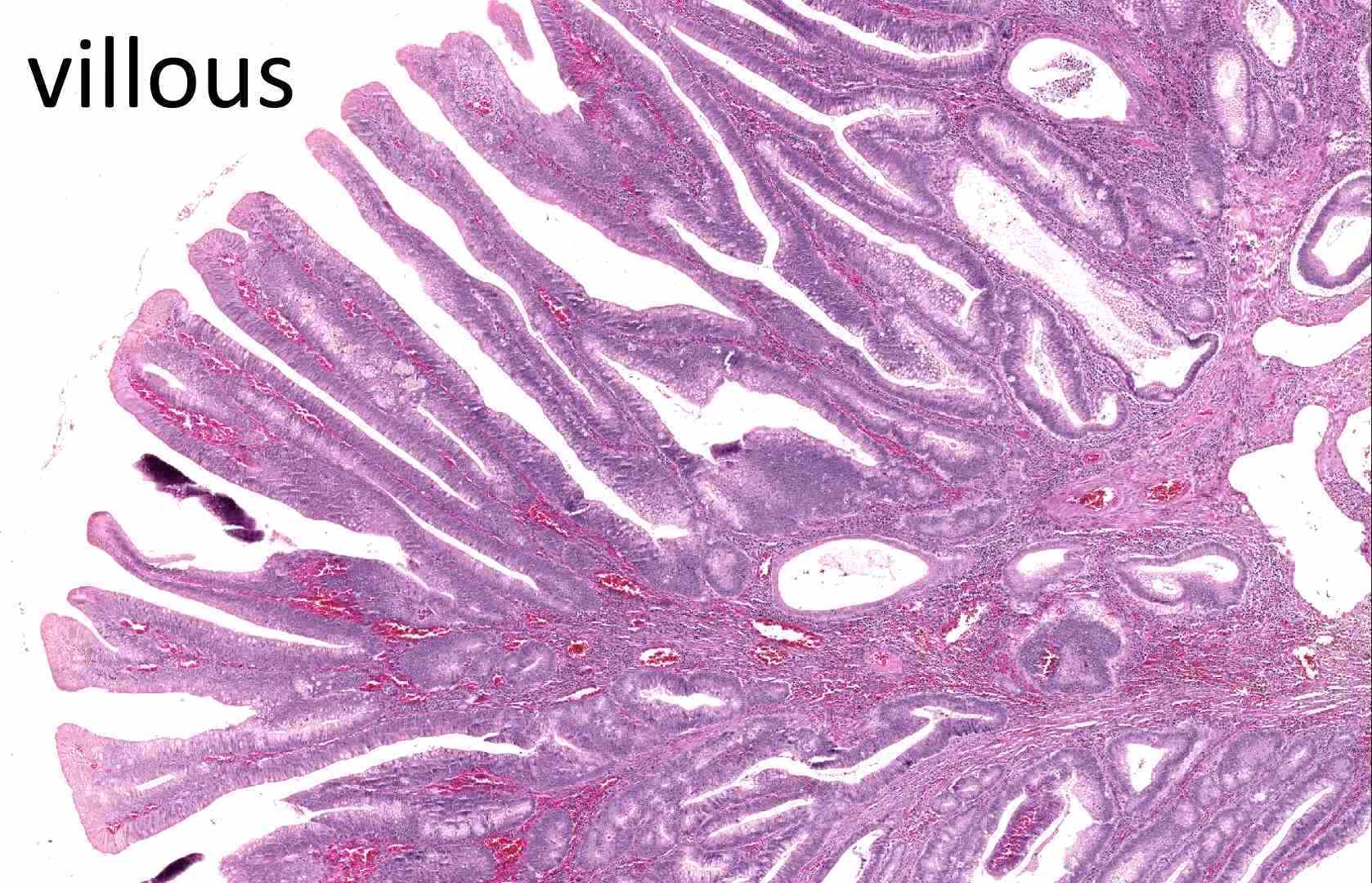
The Juan Rosai Collection [CC0], via Wikimedia Commons
Malignant Transformation
- Risk factors:
- Large size
- Sessile shape
- Villous architecture
-
Multiple adenomas
- 90% of malignancies develop from pedunculated adenomas
- 33% of Western people have benign adenomas
- 1% of adenomas undergo malignant change
- 10% of malignancies develop from sessile adenomas
- more difficult to detect
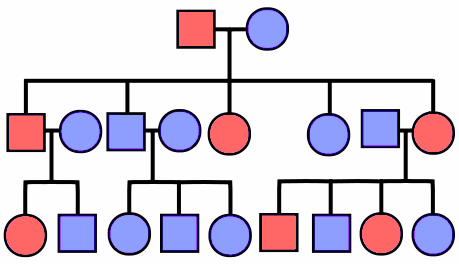
Familial Colorectal Cancer Syndromes
- Heritable genetic syndromes predisposing to polyps
- Greatly increased lifetime risks of colorectal carcinoma
- Both autosomal dominant
| Syndrome | Gene | Gene type |
|---|---|---|
| Familial Adenomatous Polyposis (FAP) | APC | Tumour suppressor |
| Hereditary Non-Polyposis Colorectal Cancer (HNPCC) |
MLH1, MSH2 | Mismatch repair |
Familial Adenomatous Polyposis (FAP)
-
3% of all colorectal carcinoma
- Develop 100s-1000s of polyps by teens
- 100% risk of carcinoma <30y if not treated by prophylactic colectomy
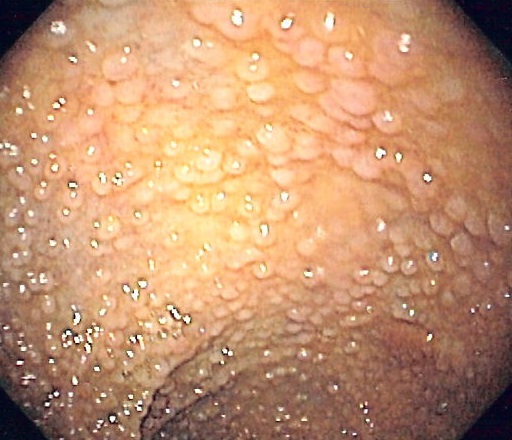
Samir [GFDLor CC-BY-SA-3.0], from Wikimedia Commons
Familial Adenomatous Polyposis (FAP)
- Adenomatous polyposis coli ( APC ) gene
- Tumour suppressor gene
- Two-hit mutation/silencing
- Specific mutation variants :
- Gardner syndrome
- Osteomas of skull and long bones
- Epidermal cysts
- Desmoid, thyroid tumours
- Supernumerary and unerupted teeth
- Turcot syndrome
- CNS medulloblastomas and glioblastomas

Hereditary Non-Polyposis Colorectal Cancer (HNPCC)
- Also called Lynch syndrome
- Cancers: colorectal, gastric, endometrial, ovarian, uterine
- Colorectal carcinoma in the young
- Inherited mutations in DNA mismatch repair genes:
- MLH1, MSH2, others (rarer)
- Two-hit mutation/silencing
- Accumulation of mutations in short, repeating microsatellite regions
Gatekeeper/Caretaker Genes
- 'Gatekeeper' genes 'control the gate' to tumour mutation
- 'Caretaker' genes 'weed the garden' of tumours
Gatekeeper
|
Control cell growth | Tumour suppressor genes | Many tumours, but less aggressive | FAP |
| Caretaker |
Stabilise genome, prevent mutations | Mismatch repair genes | Few tumours, but more agressive | HNPCC |
Molecular Pathways
- Identified pathways of colorectal carcinoma development
- Genetic and epigenetic abnormalities
- Stepwise accumulation of mutations
| Pathway | Gene | Gene type | Downstream effects |
|---|---|---|---|
| APC/β-catenin | APC | Tumour suppressor | WNT, KRAS, p53, LOH, SMAD2/4 |
| Microsatellite instability | MLH1, MSH2 | Mismatch repair | TGF-β, BAX, BRAF |
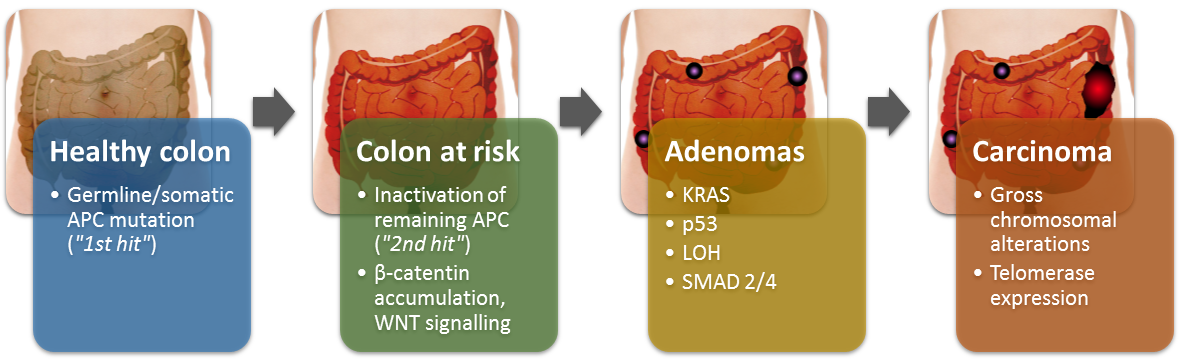
APC/β-catenin pathway
Normal APC function:
-
APC binds β-catenin, marks for degradation
Loss of APC function: - APC cannot bind, β-catenin accumulates
- β-catenin upregulates gene transcription in nucleus:
- WNT signalling pathway
- genes promoting proliferation (e.g. MYC, cyclin D1)
- Activating mutations in KRAS:
- promote growth, prevent apoptosis
- Chromosomal instability, further mutations:
- p53, LOH, SMAD2, SMAD4, gross chromosomal alterations, telomerase expansions
APC/β-catenin pathway
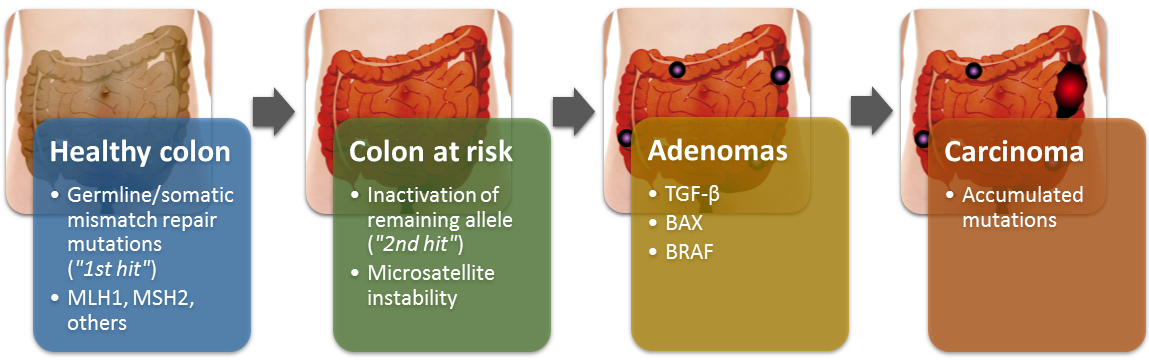
Microsatellite Instability Pathway
- Defects in mismatch repair genes
- MLH1, MSH2, others (rarer)
- Mutations accumulate in short, repeating microsatellite regions
- Regions are mostly non-coding, but contain some promoters for genes of cell growth regulation
- TGF-β: inhibits colonic epithelial cell proliferation
- BAX: pro-apoptotic for abnormal clones
- BRAF: oncogene
Microsatellite Instability Pathway
Symptoms
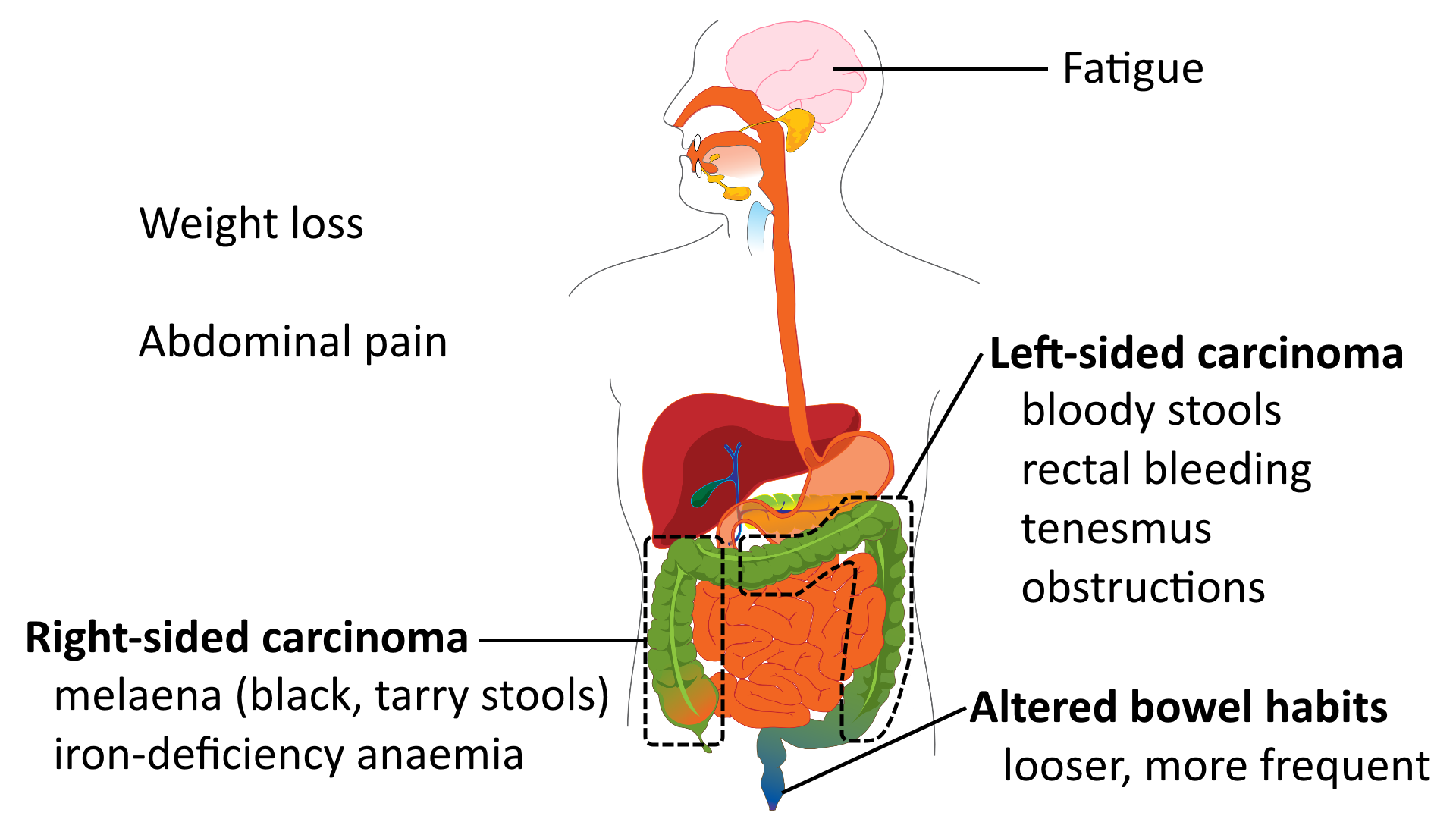
Signs

Risk Factors
- History, genes:
- Family or personal history
- Polyps, adenomas, cancers, FAP, HNPCC
-
Chronic inflammation: ulcerative colitis, Crohn's disease
-
Lifestyle: obesity, sedentary, smoking
- Diet:
- risk: fat, red meat, alcohol, refined carbs
- protective: fibre, antioxidants, NSAIDs

Age
- Strongly related, 95% of cases are >50y
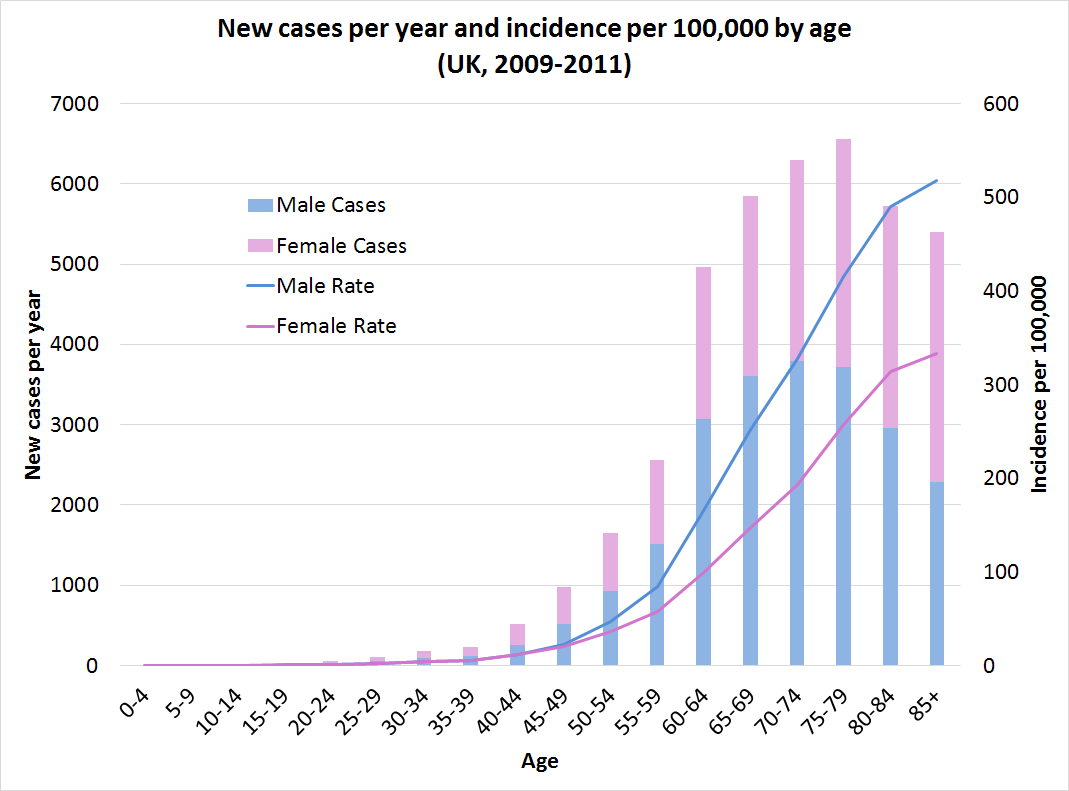
Data: Cancer Research UK
Ethnicity
-
Higher incidence in West than Africa/Asia
- Increasing incidence in Asia with Westernising diet
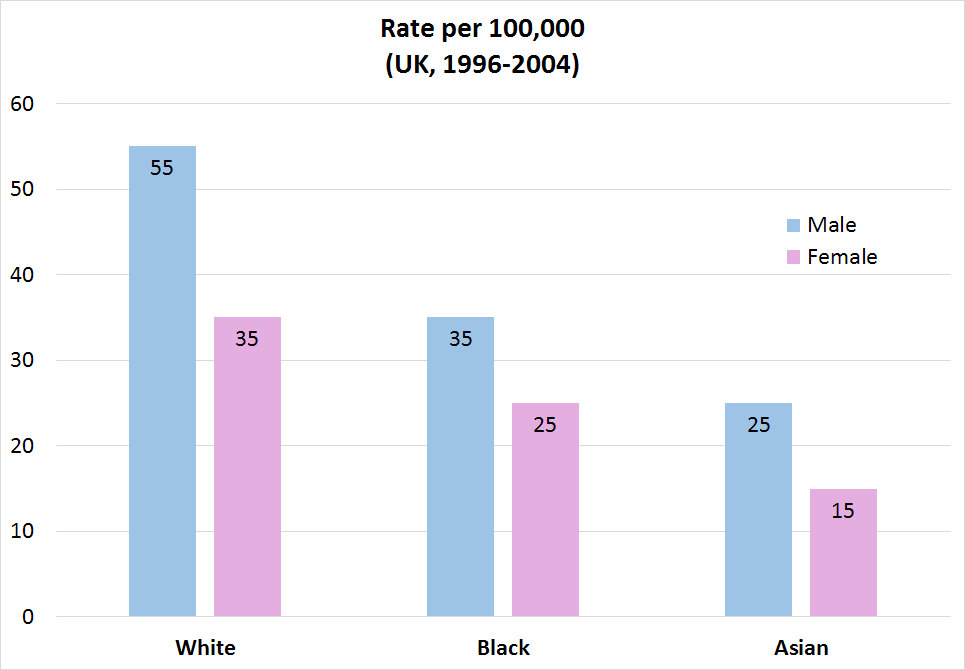
Data: Cancer Research UK
Labs
- Carcinoembryonic antigen (CEA)
- Serial measurements for follow-up
- Rising = recurrence
- Not useful for primary Dx
- Faecal occult blood
- Can detect in early stages
- Populations screening, GP, hospital
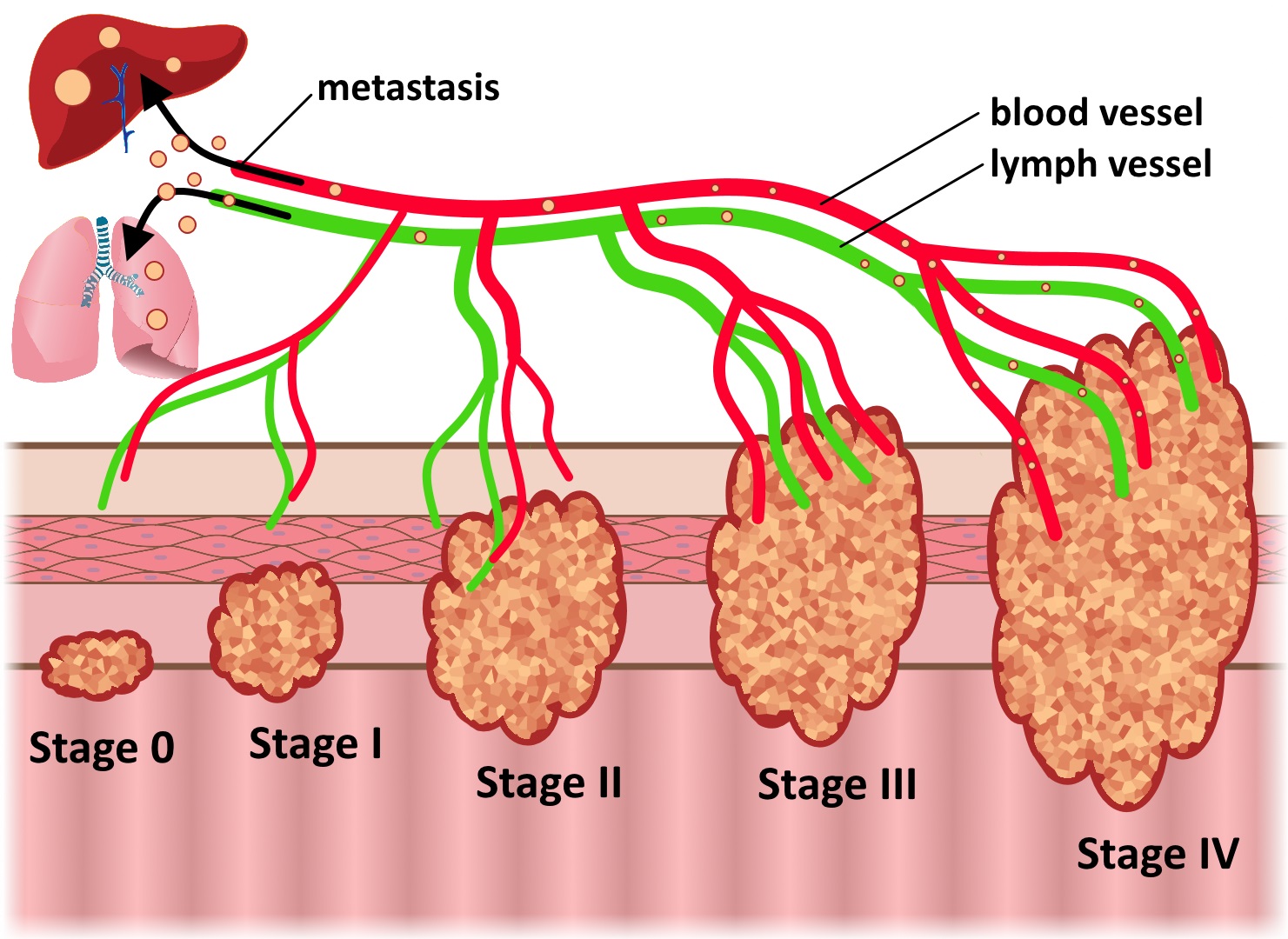
- Liver function tests (mets)
-
Haemoglobin (blood loss)


Histology
- Indicators of malignant change:
- large size
- villous architecture
- severe dysplasia
- 'Signet ring' cells (pictured →)
- Glandular cells producing mucin
- Mucin displaces nucleus to edge
- Poorer prognosis

Colonoscopy
- 'Gold-standard' diagnosis
- 70% of carcinomas in distal distal 1/3 of colon, easily visualised
- Can biopsy and remove polyps

Gilo1969 [CC-BY-SA-3.0 or GFDL], via Wikimedia Commons
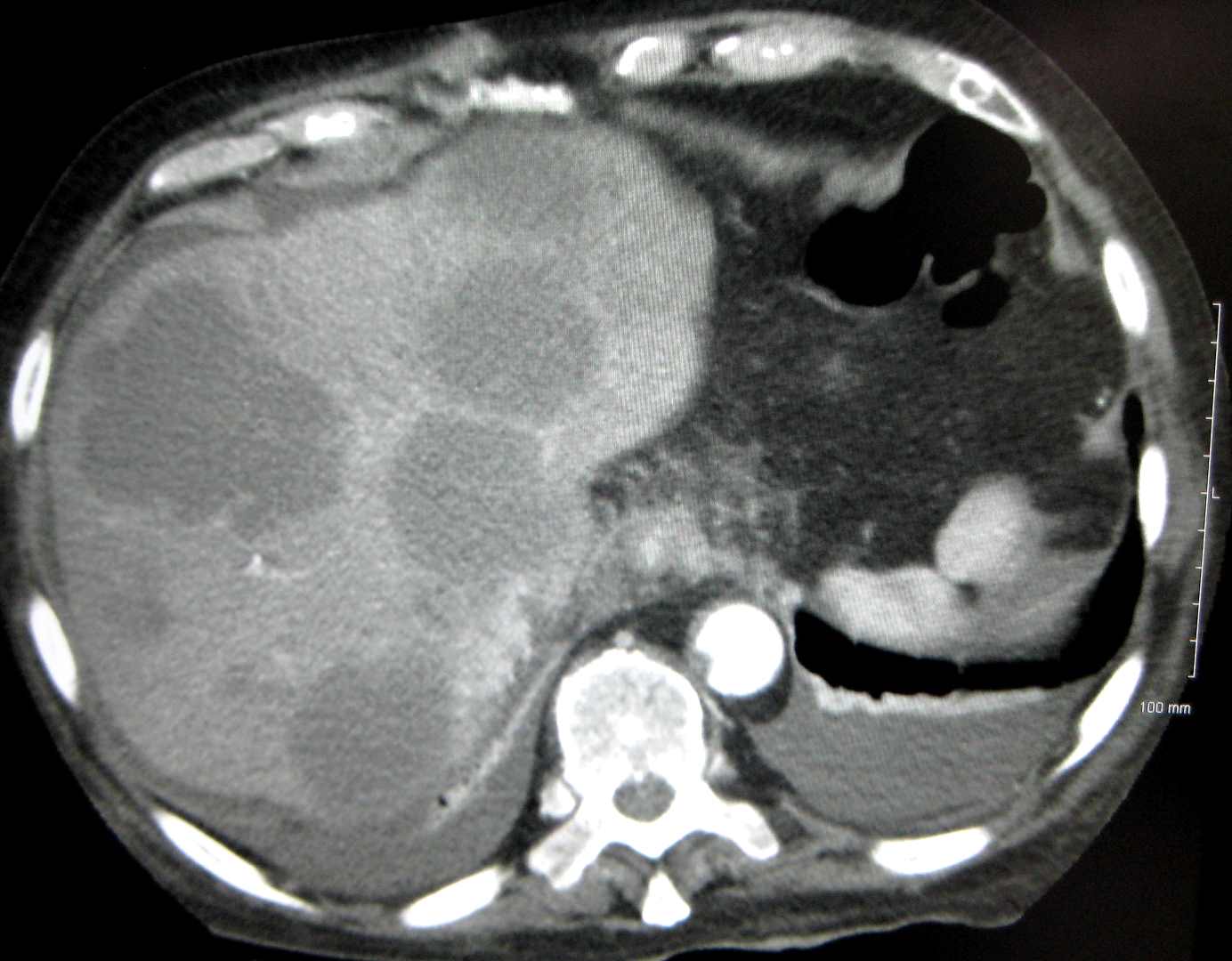
CT Colonography
- 'Virtual colonoscopy'
- Assess size, spread, metastasis
Imaging
- Ultrasound
- staging
- PET
- suspicious small lesions not confirmed by CT
- MRI
- staging, suspicious small lesions
- Double-contrast barium enema
- when CT or colonoscopy not possible
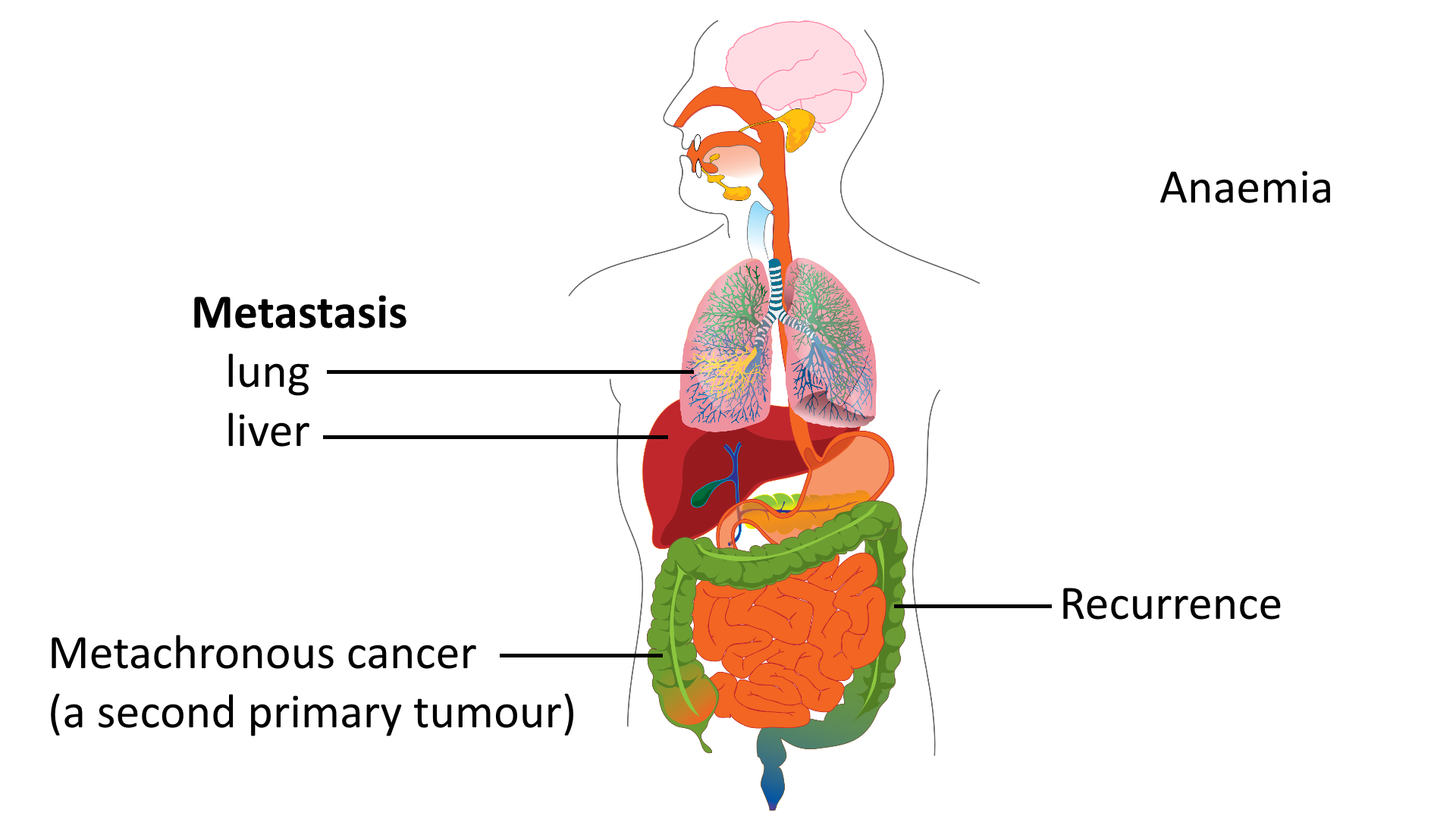
Acute Complications
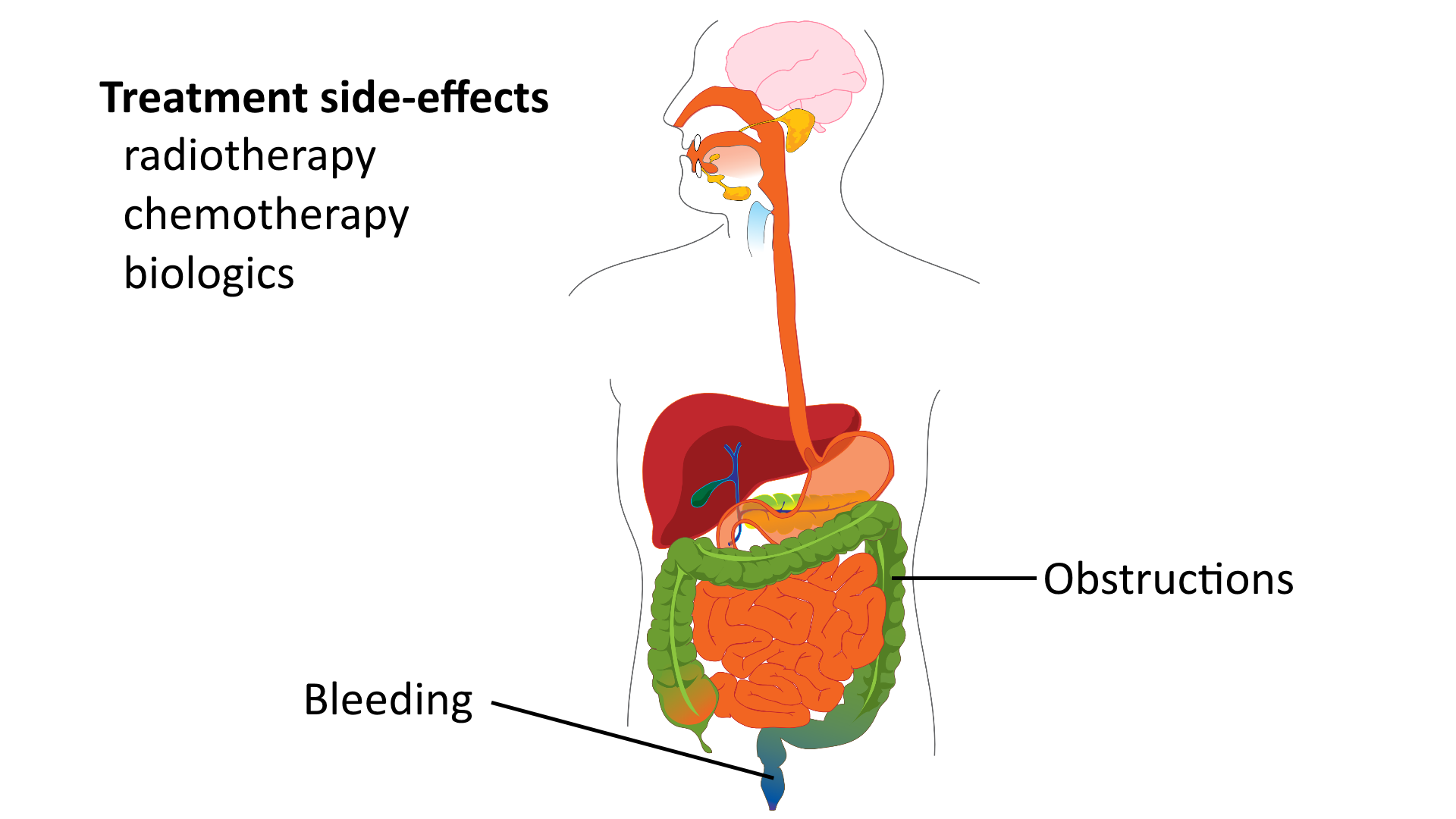
Chronic Complications
Treated
- Potential for early detection with screening
-
Removal of adenomas during endoscopy
- Most have surgery, <50% survive 5yr
- variable type, depending site
- most: resection with restorative anastomosis
- Adjuvant chemotherapy
- Biologics:
- Bevacizumab: anti-VEGF
- Cetuximab: anti-EGFR, KRAS mutation resistance

Follow-Up
- Regular colonoscopy
-
Annual CT for liver metastases
- Serial CEA, rise = recurrence
Untreated