Background on Eye Disease
PAIN (vascular Permeability, Angiogenesis, Inflammation and Neurodegeneration) are pathological hallmarks of eye diseases that culminate in blindness. The discovery and development of safe and efficacious drugs modulating these processes will significantly improve the quality of life of patients with these diseases, will reduce the associated economic burden, and enhance pharmaceutical R&D in Europe.
Angiogenesis results in the growth of new blood vessels also known as neovascularization (opens in a new window)(Ferrara and Kerberl 2005). Diabetic Retinopathy (DR) is the most common cause of blindness in people of working age in Western society and likely to increase as the population ages (opens in a new window)(Frank 2004). Type 1 and 2 diabetics develop DR characterized by retinalneovascularisation.
Overview from (opens in a new window)Sean Kirwan on (opens in a new window)Vimeo.
(opens in a new window)Diabetic Retinopathy (International) from (opens in a new window)Sean Kirwan on (opens in a new window)Vimeo.
Age-related Macular Degeneration (AMD) is a leading cause of vision loss in people aged >50 (opens in a new window)(Jageret al 2008). 90% of vision loss in AMD arises in the “wet” form, characterised by choroidal neovascularisation. These neovascular diseases result in significant socio-economic burden on the patient and state. Current therapies include laser treatment and anti-VEGFs (opens in a new window)(Zhang et al 2012). Photodynamic therapy (PDT) uses a low energy laser beam directed onto target vessels to activate a light-sensitive chemical, destroying leaky vessels. Multiple treatments are usually required and PDT cannot restore lost vision.
This video explains how AMD affects the eye and causes gradual loss of central vision. (Developed by Sean Kirwan, UCD and ICON Firecrest)
Although VEGF antibodies or aptamers (e.g. Avastin) stop the development of leaky vessels, treatment requires regular visits to the clinic for drug injection into the eye (opens in a new window)(Swinneyand Anthony 2011). Emerging therapies include anti-inflammatories (e.g. triamcinolone) and kinase inhibitors, (e. g.pazopanib) (opens in a new window)(Zhang et al 2012). The current treatments are economically unsustainable and administered invasively. From a patient’s perspective, replacement or refinement with cheaper or self-administered drugs is highly attractive.
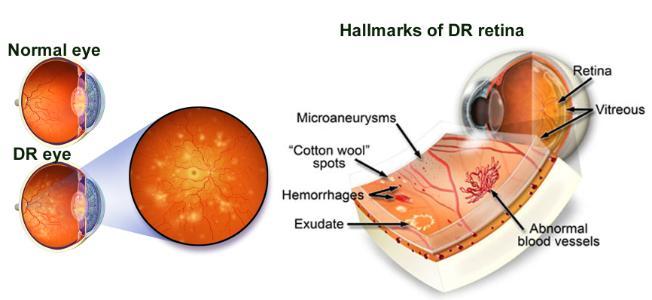
Hallmarks of Diabetic Retinopathy. (Figure: modified from Emerald Coast Eye Institute and Wikimedia Commons)
Diabetic macular oedema (DMO) arising from Retinal Vascular Permeability (RVP) is the leading cause of moderate to severe vision loss in diabetics (opens in a new window)(Klein 2007). Whilst glycaemic and blood pressure control are beneficial, effective treatments for DMO remain an unmet clinical need. Laser photocoagulation and intravitreal antibodies to VEGF are only effective in around 50% of DMO patients. Again, these treatments are highly invasive and place a huge burden on both patients and health care resources. Development of an orally available therapeutic for DMO would have an enormous impact. Since DMO is a chronic disease, systemic inhibition of anti-VEGF is not a viable approach. Consequently, a growing R&D focus is on VEGF-independent interventions.
In the anterior eye, opacity (due to ulceration, scarring or corneal stem cell deficiency), inflammation and/orneovascularisation of the cornea can result in blindness (opens in a new window)(Williams et al 2013). A severe situation is the rejection of ocular tissues transplanted to reconstruct an ocular surface. This transplant type has a failure rate of >40% due to severe basal inflammation in the host tissue. Current treatments address tissue repair, but not the out-of-control inflammation that perpetuates a destructive vicious cycle. In addition, defective tissue repair can lead toneovascularisation. Thus, novel inhibitors of corneal vascularisation and inflammation, preferably by eyedrop delivery, will enhance patient compliance and treatment.
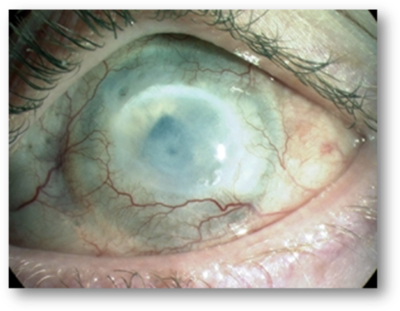 Cornea Injured by Chemical Burn which has Developed Opacity & Neovascularisation. Author: Secker, G.A., and Daniels, J.T., Limbal Epithelial Stem Cells of the Cornea (June 30, 2009), Stembook (through Wikimedia Commons).
Cornea Injured by Chemical Burn which has Developed Opacity & Neovascularisation. Author: Secker, G.A., and Daniels, J.T., Limbal Epithelial Stem Cells of the Cornea (June 30, 2009), Stembook (through Wikimedia Commons).
In the eye, neurodegeneration of photoreceptors or inner retinal neurons, and atrophy of the retinal pigment epithelium (RPE) or cornea, are hallmarks of AMD, DR or CI and of other significant forms of blindness including retinitis pigmentosa and glaucoma (opens in a new window)(Zhang et al 2012). Numerous factors have been reported to protect ocular cells from death including growth factors (e.g. CNTF), histone deacetylase inhibitors (e.g. valproic acid) and serotonin receptor agonists (e.g. AL-8309A) which are in clinical trial. However, safe and effective compounds have not been clinically developed to date and thus there is an unmet clinical need for oculoprotective drugs.