Metronomic chemotherapy shows therapeutic benefits in preclinical cancer models
UCD researchers with international colleagues have demonstrated for the first time that lowering chemotherapy doses can improve tumour oxygenation and decrease HIFα levels in animal models of colon and breast cancer, associated with significant pre-clinical benefits.
Hypoxia is a common feature of most solid cancers. It arises as a mismatch between cellular oxygen demand and supply. Hypoxia is associated with unfavourable chemotherapeutic responses, recurrence, and cancer cell metastasis.
Conventional chemotherapy is a systemic treatment for many cancers. It relies on administering therapeutics at the maximum tolerated dose to massively eliminate cancer cells over a relatively short period of time.
Nevertheless, this treatment can further increase hypoxia, while creating microenvironmental conditions that enable cancer cell regrowth and metastasis, in addition to causing toxic side effects.
By contrast, low‐dose, frequent, and regular administration of chemotherapy drugs causes fewer adverse effects, while displaying therapeutic benefits in a variety of preclinical models of cancer. This is often referred to as metronomic chemotherapy.
The research team from UCD, Sunnybrook Research Institute, Toronto and University of Toronto performed the first quantitative side‐by‐side comparison of metronomic and conventional chemotherapies on tumoral hypoxia and hypoxia‐inducible factors (HIFs).
HIFs are a family of master transcriptional regulators (or group of proteins) exerting multiple functions on many aspects of cancer biology, including therapy resistance, metastasis, and mortality.
The team found that metronomic chemotherapy dramatically improves tumour oxygenation, while offsetting HIF induction caused by conventional chemotherapy in preclinical models of metastatic colon and breast cancers. 
Picture 1. Conventional chemotherapy activates a master oxygen switch, known as hypoxia-inducible factor-1α (HIF-1α seen as brown staining), in experimental colon cancers spread to the liver (left photo). Switching to a continuous low-dose (metronomic) therapeutic schedule prevents the increase of HIF-1α (right photo), leading to improved pre-clinical outcomes.
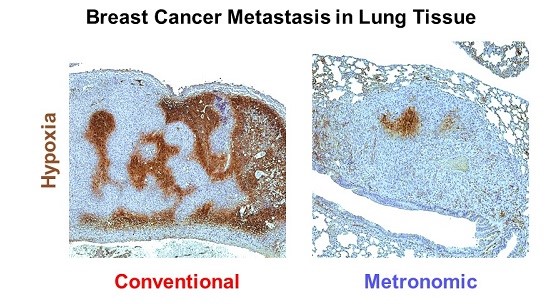
Picture 2. In a second model of disseminated breast cancer, conventional chemotherapy severely impairs tumoral oxygenation (a condition known as hypoxia, seen as brown staining), predicting resistance to therapy and shortened survival. In contrast, continuous low-dose (metronomic) chemotherapy, significantly increases oxygen levels (shown as a decrease in brown staining; right photo). Photographs illustrate disseminated breast cancer as it grows within the lungs.
In addition, the team developed two compact, 11‐gene signatures that allow a simplified estimation of HIF levels in colon and breast cancers, which might be helpful to identify patients more likely to benefit from metronomic therapies.
Dr Luana Schito and Dr Sergio Rey carried out a significant amount of the work leading to this publication since moving to Dublin last year. They are both Lecturers/Assistant Professors (Ad Astra Fellows) in UCD School of Medicine and Fellows, UCD Conway Institute.
Describing the impact of the findings, they said, “These results provide a rationale for using metronomic chemotherapy as a maintenance strategy to improve oxygenation and decrease cancer dissemination in two of the most common types of cancer. It gives clinicians another tool aimed at improving survival in patients with hypoxic cancers, possibly by combining metronomic chemotherapies with novel compounds capable of directly targeting HIFs.”
The open access publication in EMBO Molecular Medicine is available online: https://www.embopress.org/doi/full/10.15252/emmm.201911416
Schito L, Rey S, Xu P, Man S, Cruz-Muñoz W, Kerbel RS. Metronomic chemotherapy offsets HIFα induction upon maximum-tolerated dose in metastatic cancers. EMBO Molecular Medicine 12: e11416, 2020 - PMID: 32686360. https://doi.org/10.15252/emmm.201911416
Social Media Links